




Abstract
Osteoarthritis (OA) is an important cause of pain, disability and economic loss in humans, and is similarly important in the horse. Recent knowledge on post-traumatic OA has suggested opportunities for early intervention, but it is difficult to identify the appropriate time of these interventions. The horse provides two useful mechanisms to answer these questions: 1) extensive experience with clinical OA in horses; and 2) use of a consistently predictable model of OA that can help study early pathobiological events, define targets for therapeutic intervention and then test these putative therapies. This paper summarises the syndromes of clinical OA in horses including pathogenesis, diagnosis and treatment, and details controlled studies of various treatment options using an equine model of clinical OA.
Introduction
Osteoarthritis (OA) is the most common disease affecting the joints in humans and among the most important causes of pain, disability and economic loss in all populations.1-3 In 2008 it was estimated that nearly 27 million adults in the United States have clinical OA (up from the estimate of 21 million for 1995).4 There are also estimates of 100 million people with OA in the European Union.5 The physical impairment caused by OA of a single lower extremity joint has been compared with that caused by end-stage kidney disease or heart failure.6 It has also been estimated that even with the best current care of significant joint injuries, the risk of post-traumatic OA ranges from about 20% to more than 50%.7 There have been a number of studies in human post-traumatic OA demonstrating that OA occurs frequently in people who suffer a significant joint injury. In one study of 1321 former medical students it was found that 14% of those who had a knee injury during adolescence and young adult life developed OA of the knee, compared with 6% of those who did not have a knee injury.8 Follow-up data of people who suffered ligamentous and meniscal injuries of the knee demonstrated that a ten-fold increase risk of OA as compared with those that did not have a joint injury.9,10 Another study showed that between 33% and 44% of patients sustaining articular fractures of the knee develop knee OA.11
More recent knowledge on post-traumatic OA has suggested opportunities for early intervention, based on the concept that impact joint injuries initiate a sequence of biological events causing the progression of joint degeneration, which then leads to post-traumatic OA.1 The comprehension of the time frame of these pathobiological events has been helped by in vitro and in vivo animal studies,1,2,12-14 which have provided evidence that new molecular interventions can mitigate or even possibly arrest these developments, thereby preventing progressive degeneration of the joint. While it is difficult to confirm the ideal time for such early interventions in human OA, the horse potentially provides two useful mechanisms to answer these questions, including: 1) extensive experience with clinical OA in horses12,15; and 2) use of a consistently predictable model of OA that can help study early pathobiological events, define targets for therapeutic intervention and then test these putative therapies, as will be detailed below.
Osteoarthritis in the horse
Spontaneous joint disease is a common clinical problem in the horse.16,17 Surveys estimate that up to 60% of lameness is related to OA.17,18 It has been observed by Koch and Betts19 that human OA is not a well-defined entity, in that pathologists define OA on a structural basis20 and epidemiologists define OA based on pain.21 The situation is similar in horses, where the clinical importance has been emphasised by a large United States Department of Agriculture (USDA) survey of lameness in the horse (defined as an abnormality of gait such that the horse cannot be used for its intended purpose or could only be used if intervention [such as medication, corrective shoeing or rest] was employed), which found that lameness was because of a leg or joint problem in approximately 50% of cases.17 On the structural side however, a number of pathological studies in the metacarpophalangeal joint (an important high-motion joint) of the horse have been published recently22-24 and objective parameters of macroscopic and microscopic examination of clinical OA as well as experimental OA have been defined.13
Equine degenerative arthritis was first reported in 1938 and the pathological changes were compared with human OA.25 Although examination of osteo-arthritic joints were initially limited to morphological observations,25-29 equine OA received its first clinical attention at the American Association of Equine Practitioners in 1966, and its relationship with lameness and ‘use trauma’ became a central aetiologic concept.12,14 By 1975 articular cartilage lesions were considered the indispensable criteria of OA but it was also recognised that they may not be the centrally important cause of clinical disease. Today equine OA may be considered as a group of disorders characterised by a common end stage: progressive deterioration of the articular cartilage accompanied by changes in the bone and soft tissues of the joint.12 This definition is simpler but comparable with one created for human OA at a workshop sponsored by the American Academy of Orthopaedic Surgeons, The National Institute of Arthritis, Musculoskeletal, and Skin Diseases, The National Institute on Aging, The Arthritis Foundation and The Orthopaedic Research and Education Foundation, where OA was redefined as: ‘a group of overlapping distinct disease which may have different etiologies, but with similar biologic, morphologic, and clinical outcomes. Disease processes do not only affect the articular cartilage but also involve the entire joint, including the subchondral bone, ligaments, capsule, synovial membrane and peri-articular tissues. Ultimately the articular cartilage degenerates with fibrillation, fissures, ulceration, and full thickness loss of the joint surface.’30 It has now been recognised that the equine OA disease process can start with disease in synovial membrane, fibrous joint capsule, subchondral bone and ligaments as well as articular cartilage or be a combination of the above.12
The metacarpophalangeal (MCP) joint is the most common joint for spontaneous OA in the racehorse, followed by the carpal joints. Both joints have close fitting articular surfaces that can quickly develop linear erosions and wear lines in association with osteochondral fragmentation. In the last ten to 15 years, improvements in arthroscopic techniques and a higher competitive standard in Western Performance equestrian events have resulted in a new spectrum of femorotibial traumatic disease and OA, which has much analogy to human OA of the knee. OA can occur early in equine athletes or later in older horses.31-33 An arthroscopic grading system has been used for clinical disease in high motion joints34,35 and biomarkers related to macroscopic and histological cartilage lesions have been evaluated.36,37
How can the equine joint tissues be injured or insulted?
The risk factors for development of OA in humans has been classified into two fundamental mechanisms related either to the adverse effects of ‘abnormal’ loading on ‘normal’ cartilage or of ‘normal’ loading on ‘abnormal’ cartilage,2 and similar pathways have been described in horses (Fig. 1).12 The reaction in various joint-associated tissues should not be considered in isolation. For example, in the carpus of a racehorse, considerable damage may be inflicted directly to the articular cartilage and regions of concussion by cyclic fatigue damage (as exemplified by fractures and chondral lesions un-associated with fracture), and there is often primary damage to the subchondral bone other than fracture that often leads to fracture or secondary damage to the articular cartilage from either loss of support or release of cytokines. Subchondral sclerosis has also been proposed as leading to further physical damage in the articular cartilage because of decreased shock absorption, but this has not been proven. Acute synovitis and capsulitis is the most common problem in these same joints and may contribute to the degradative process in articular cartilage by the release of enzymes, inflammatory mediators and cytokines (Fig. 2).14,38
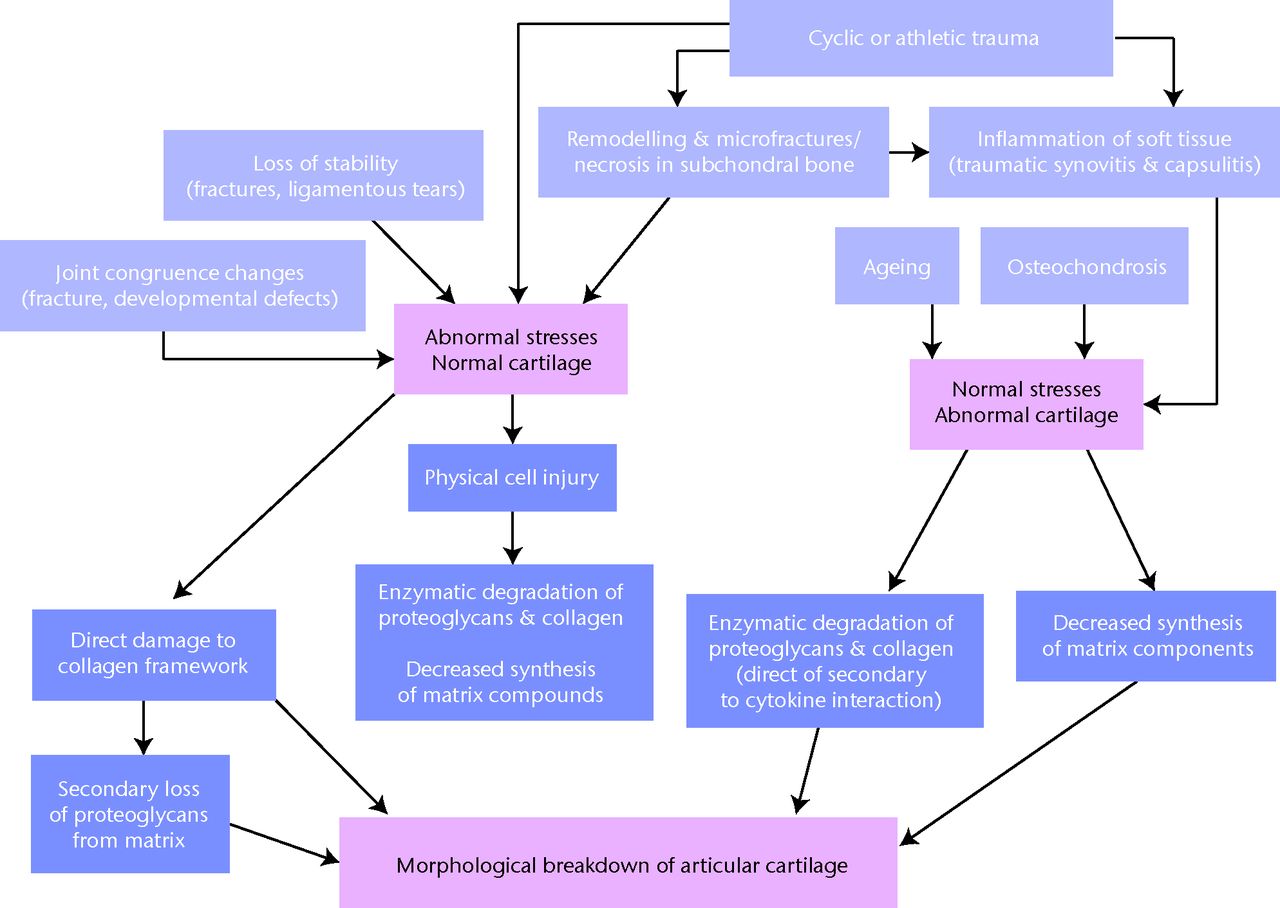
Fig. 1
Diagram showing the possible pathways for degradation of articular cartilage secondary to joint trauma in the horse (reproduced with permission from McIlwraith CW. Frank Milne Lecture: from arthroscopy to gene therapy: 30 years of looking in joints. Am Assoc Equine Pract 2005;51:65–113).
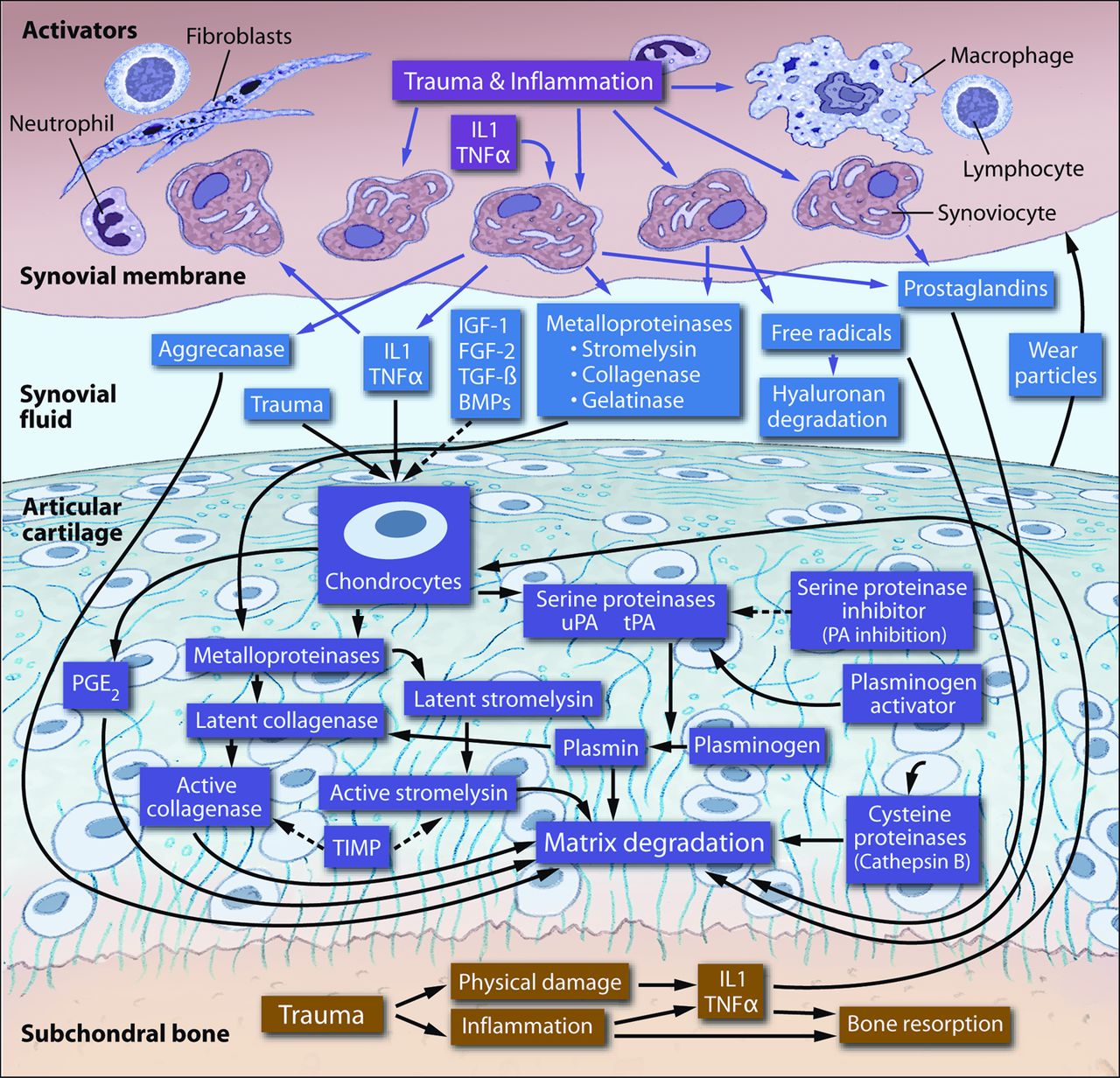
Fig. 2
Diagram showing the factors involved in enzymatic degradation of articular cartilage matrix, Dotted lines indicate factors that may inhibit degradation (IL1, interleukin-1; TNFα, tumour necrosis factor-α; IGF-1, insulin-like growth factor-1; FGF-2, fibroblast growth factor-2; TGF-β, transforming growth factor-β; BMPs, bone morphogenetic proteins; PG, prostaglandin; PLA2, phospholipase A2; uPA, urokinase plasminogen activator; tPA, tissue plasminogen activator; PA, plasminogen activator; PGE2, prostaglandin E(2); TIMP, tissue inhibitor of metalloproteinases) (reproduced with permission from McIlwraith CW. Frank Milne Lecture: from arthroscopy to gene therapy: 30 years of looking in joints. Am Assoc Equine Pract 2005;51:65–113).
A common feature of joint injury leading to human post-traumatic OA is the sudden application of mechanical force (impact) to the articular surface, and it has been proposed that the extent of mechanical damage to any structures is a function of the intensity of the impact.1 Injury and responses range from damage to cells and matrices without macroscopic structural disruption to displaced fractures through cartilage and bone.39-41 While it has been pointed out that hypotheses concerning the relationship between joint injuries and the biological events that lead to progressive joint degradation cannot be tested in human patients,1 such events can be looked at more closely with equine OA models.
The significance of synovial membrane inflammation in the pathogenesis of equine OA was demonstrated in an early experimental model by the first author.42 This induced synovitis model using filipin demonstrated that cartilage degradation could occur in the absence of instability or traumatic disruption of the tissues and loss of glycosaminoglycan (GAG) staining was associated with early morphologic breakdown of the surface of the cartilage and loss of GAG staining throughout the ECM. Since then it has been recognised and demonstrated in various experiments that synovitis (and capsulitis) is important as it produces pain and discomfort in the horse as well as increased production of mediators that can contribute to the osteo-arthritic process, including metalloproteinase (MMP), aggrecanases, prostaglandins, free radicals as well as interleukin-1 and tumour necrosis factor-α (TNFα).42-50 A recent paper on cytokine and catabolic enzyme expression in synovium, synovial fluid and articular cartilage of naturally osteo-arthritic equine carpi showed that TNFα was abundantly expressed in synovial membrane and cartilage, compared with IL-1β being over expressed in OA cartilage but not to a significant extent in synovium.51 Expression of ADAMTS-5 and MMP-13 was also significantly increased in synovial tissue and ADAMTS-4 and MMP-13 also were significantly expressed in OA cartilage.
The role of equine IL-1 in producing OA in the equine carpus was well demonstrated by total inhibition of OA production by gene therapy with IL-1ra.50,52 Interleukin-1β has been called the master cytokine in human OA,53 and while TNFα is thought to be the most prominent cytokine in the acute stages of human OA, IL-1β remains high throughout all stages.54 A recent paper evaluating gene expression in synovial tissue samples obtained from 12 patients with OA and 32 patients undergoing total knee replacement showed that there was no significant difference in the expression levels of MMPs, interleukin-1β of TNFα mRNA.55 The simple overall picture for the master role of Il-1 is illustrated in Figure 3. It has been recently reported that low innate production of interleukin-1β and interleukin-6 is associated with the absence of human OA in old age.56
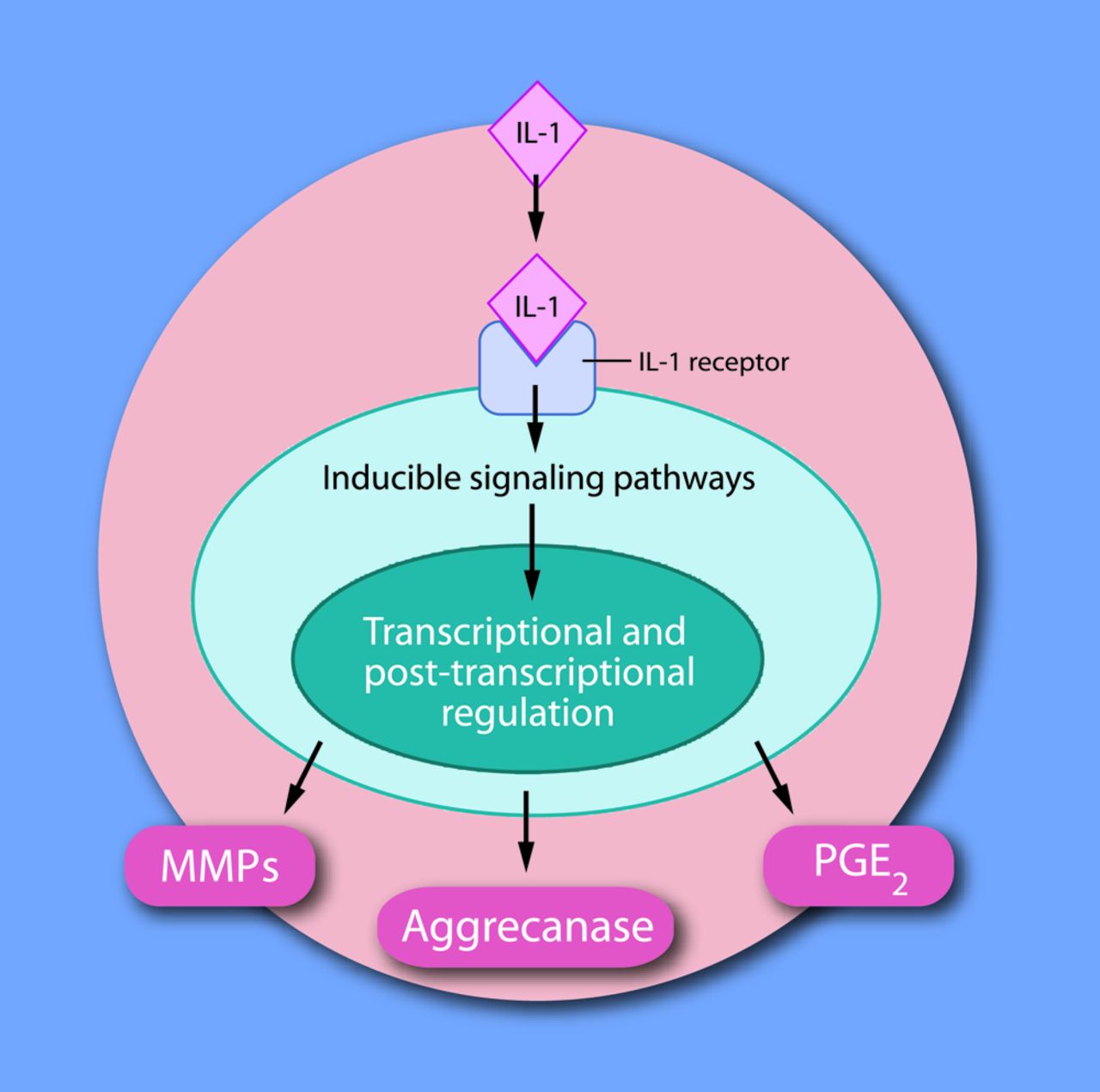
Fig. 3
Diagram of interleukin-1 (IL-1) activating matrix metalloproteinases (MMPs), aggrecanase and prostaglandin E2 (PGE2) release acting through IL-1 receptors on the cell membrane (reproduced with permission from McIlwraith CW. Frank Milne Lecture: from arthroscopy to gene therapy: 30 years of looking in joints. Am Assoc Equine Pract 2005;51:65–113).
The role of synovitis in the pathophysiology and production of clinical symptoms of human OA was recently reviewed.57 Gradual emergence of recognition of synovitis in human OA has brought the human and equine entities into closer alignment as synovitis is invariably present in all OA entities in the horse.12,46 Proper balance of anabolic and catabolic activities is crucial for the maintenance of cartilage integrity and for the repair of molecular damage sustained during daily use.58 Recognition that the balance of anabolic and catabolic activities is compromised in OA has led to various efforts of therapy to both promote anabolism as well as inhibit catabolism. While the anti-catabolic effects of equine interleukin-1 receptor antagonist (IL-1ra) gene therapy50,52 has clearly demonstrated its ability to prevent or decrease the development of equine OA, another study by the same authors demonstrated that repair of articular defects could be enhanced by the combination of IL-1ra and IGF-1 gene therapy.59
Diagnosis of naturally occurring joint injury and osteoarthritis
Clinically the disease is characterised by varying levels of lameness, the presence of synovial effusion, soft-tissue swelling and response to flexion. The main radiological features include osteophytes and increased subchondral bone density (with occasional lysis or cyst-like lesions in the subchondral bone) and end-stage joint space reduction. Cartilage defects can be seen on MRI with various levels of signal change in the subchondral bone. Osteophytes in human OA have more recently been classified as marginal (at the periphery of the osteochondral junction) or central (growing from the subchondral plate into the cartilage). Central osteophytes are typically found in joints with marginal osteophytes and in advanced and symptomatic knee OA,60,61 and are consistently associated with overlying cartilage defects.61 A recent study in our laboratory described histological lesions of severe subchondral bone remodelling invading the cartilage in horses.24 Central osteophytes have not been recognised in clinical cases in the horse until very recently.62 Abnormalities consistent with central osteophyte formation were demonstrated on MRI (SPGR Sequence) in seven of 20 (35%) paired metacarpophalangeal joints. They were identified as focal, hypointense protuberances from the subchondral plate into the cartilage and microscopically consisted of dense bone protruding into the calcified cartilage and disrupting the tide marks and were consistently associated with overlying cartilage defects.62 Arthroscopic evaluation remains the gold standard for defining the degree of osteo-arthritic disease (Fig. 4).
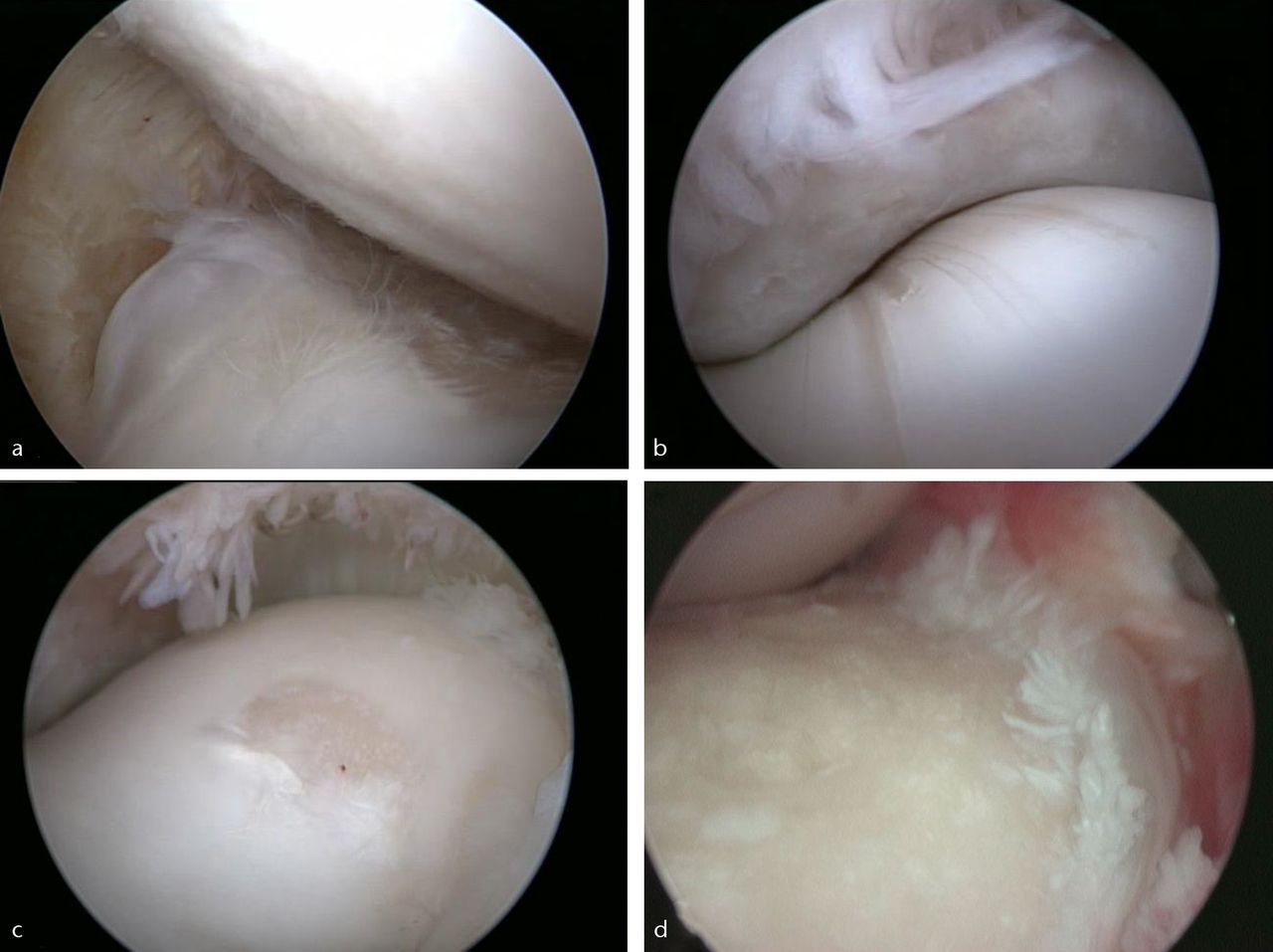
Fig. 4
Arthroscopic images of a) the medial aspect of middle carpal joint, showing erosion of articular cartilage and osteophytosis on radial carpal bone, and minor cartilaginous disease on the opposing surface of the third carpal bone, b) the metacarpophalangeal joint, showing wear line formations signifying early osteoarthritis on the distal metacarpus, c) the metacarpophalangeal joint, showing focal cartilage erosion on the medial condyle of the distal metacarpus, and d) the middle carpal joint, showing severe erosion of articular cartilage on the distal radial carpal bone.
Evaluation of treatments for OA
Pain and limited function are the primary reasons for OA patients to seek treatment, but few options exist beyond pain management and prescription of mobility aids.63 The same authors discuss the different stages of OA including clinically silent, active (equals ‘inflamed’) or clinically manifest, decompensated OA with continuous pain that all require different therapeutic measures. The pharmacological treatment of OA has evolved to becoming more evidence-based but publication bias, pharmaceutically vested interest and complete search databases and deliberate selectivity of data presented may have an impact on meta-analyses.63 For example, trial patients are commonly drawn from hospital practice, from which results may not be able to be directly extrapolated to primary care or pharmacy sales. The European League Against Rheumatism (EULAR) produced recommendations for therapy of hip and knee OA, based on evidence based evaluation of clinical studies and the opinions of experts from 12 European countries.64,65 Also, the American College of Rheumatology (ACR) published recommendations for the therapy of hip and knee OA based on a consensus between four OA experts from the United States.66 Very similar recommendations were created by the ACR and EULAR. Chard, Tallon and Dieppe67 were particularly critical of 94% of 930 scientific publications being judged positively, despite being unsupported by statistically significant study results.
The gold standard for determining the benefit of many therapeutic compounds in human rheumatology is the use of large randomised, blinded and placebo controlled trials. While many such studies have been performed and reliable meta-analyses have been done,68 most data from such studies have relied on symptomatic outcome measures. The difficulties in undertaking human clinical trials in the pursuit of a disease modifying osteo-arthritic drug (DMOAD) have been recently summarised and the need for a new development paradigm for DMOAD emphasised.69 The use of radiology to determine joint space, which is the only accepted structural endpoint in OA trials, is associated with a series of concerns including the inherent inability to visualise cartilage, the insensitivity of radiographs to detect early and small changes and the slow progression of OA being a common finding in clinical trials of OA. In one study only 13% of the untreated OA patients qualified as structural progressors (defined as having joint space narrowing ≥ 0.6 mm over a two year period).70
The ideal therapeutic agent for equine OA would be an agent that both relieves the symptoms of lameness (symptom-modifying OA drug, or SMOAD) as well as producing disease modifying effects (DMOAD). Evaluating treatments in clinical equine cases has the same challenges as human OA and only recently have there been any reasonable quality randomised control trials investigating the efficacy of articular therapeutics.71-74 Again these studies were associated with identifying SMOAD effects rather than any disease-modifying activity of the drug. The problems associated with performing high-quality randomised, controlled studies and the lack of well-validated outcome measures determining disease-modifying activity in vivo make the use of equine experimental studies appropriate. They have provided considerable objective information on therapies (described below) as well as enabled validation of imaging as well as synovial fluid and serum biomarkers to define DMOAD activity.75-77
A recent paper concluded that there was a major need for more responsive outcome measures for both symptom and structure modifying agents for human OA and a need to focus on developing and qualifying biomarkers to enable the development of DMOADs.78 The author cited a need to develop pre-clinical models that are more predictive of human OA progression, or accept the risks associated with advancing compounds in development that demonstrate moderate results in already established models of OA.78 Animal model systems represent an important adjunct and surrogate to studies of OA in humans. They provide a means to study the pathobiology of OA as well as aid in the development of therapeutic agents and biological markers for diagnosing and prognosing the disease.79 In addition, OA can be a major clinical challenge in animals, particularly the athletic horse. A number of experimental models of OA have been developed and used in the horse (Table I),42,47,50,76,77,80-103 but many have deficiencies with inconsistency in the level of disease between animals, as well as appropriateness to naturally occurring OA in the horse.13 In addition, models based on instability commonly do not represent the clinical situation in man. The most commonly published model is the arthroscopically created osteochondral fragment-exercise model developed at Colorado State University (CSU), which is not an instability model.47,50,76,77,93-97,103
Table I
Experimental models of OA that have been described in the horse (reprinted with permission from McIlwraith et al. The OARSI histopathology initiative: recommendations for histological assessments of osteoarthritis in the horse. Osteoarthritis Cartilage 2010;18:S93–S105)
| Type of model | Specific name |
|---|---|
| Intra-articular injection of chemicals | Filipin42,80 |
| Sodium monoiodoacetate81-83 | |
| Amphotericin84 | |
| Escherichia coli lipopolysaccharide85-87 | |
| Interleukin-188 | |
| Polyvinylalcohol foam particles89 | |
| Carrageenan90 | |
| Instability | Carpal fracture91 |
| Cutting collateral & collateral sesamoidean ligaments in metacarpophalangeal joint92 | |
| Osteochondral fragmentation and exercise | Carpal osteochondral fragment – exercise model47,50,76,77,79,93-97 |
| Trauma | Single impact on medial femoral condyle98 – progresses to focal defects and OA |
| Disuse | Lower limb cast immobilisation100-102 |
The equine carpal osteochondral fragment model of OA
This model mimics clinical equine OA relevant to horses and has relevance to human OA,50,96 and involves creating an 8 mm fragment on the distal dorsal aspect of the radial carpal bone.13 The model induces progressive OA without producing severe lameness.47,50,76,77,93-97,103 The macroscopic and histological evaluations have been presented recently.13 Both longitudinal synovial fluid and imaging biomarker changes have been detailed.76,77 Recently an equine model of post-traumatic OA in the medial femorotibial joint has been described.98 The articular cartilage in this joint is similar to the human knee,99 but the model has not yet been sufficiently investigated to evaluate its overall value as translational research regarding medications, where the carpal osteochondral model has.
Power calculations for clinical gross and histological outcome parameters have led to a total of 16 skeletally mature horses (aged between two and five years) being used in a typical study.50 Horses are in good health without palpable effusion or radiological abnormalities and free of lameness before and after joint manipulation. The horses are divided into two equal groups, treated or control. An 8 mm osteochondral fragment is created on the distal-dorsal aspect of the radial carpal bone (equivalent to human scaphoid)105 in one randomly chosen mid-carpal joint of each horse to produce an experimental OA, and the opposite joints serve as the control (Fig. 5). Exposed subchondral bone between fragment and parent bone are debrided using a motorised arthroburr to form a 15 mm wide defect bed (Fig. 5). The size, location of the fragment, loss of bone and the subsequent synovitis mimic naturally occurring equine OA as clinical cases of osteochondral fragmentation in this location, if left untreated, typically progress quickly in developing OA symptoms and lesions. Diagnostic arthroscopy is also performed on the contralateral mid-carpal joint to confirm the absence of any significant lesions.34 After surgery all horses are housed in 3.65 m × 3.65 m stalls and exercise on a high-speed treadmill begins on day 14 after fragment creation, and continues five days per week until day 70, simulating athletic conditions commonly seen in horses developing osteochondral fragmentation and subsequent OA. Institution of treatment depends on what is being studied but if it is an intra-articular medication the first (or sometimes only) injection is given at day 14. This model has been used to evaluate different treatment modalities for equine OA in blinded, controlled studies and described below.47,50,93-97,103
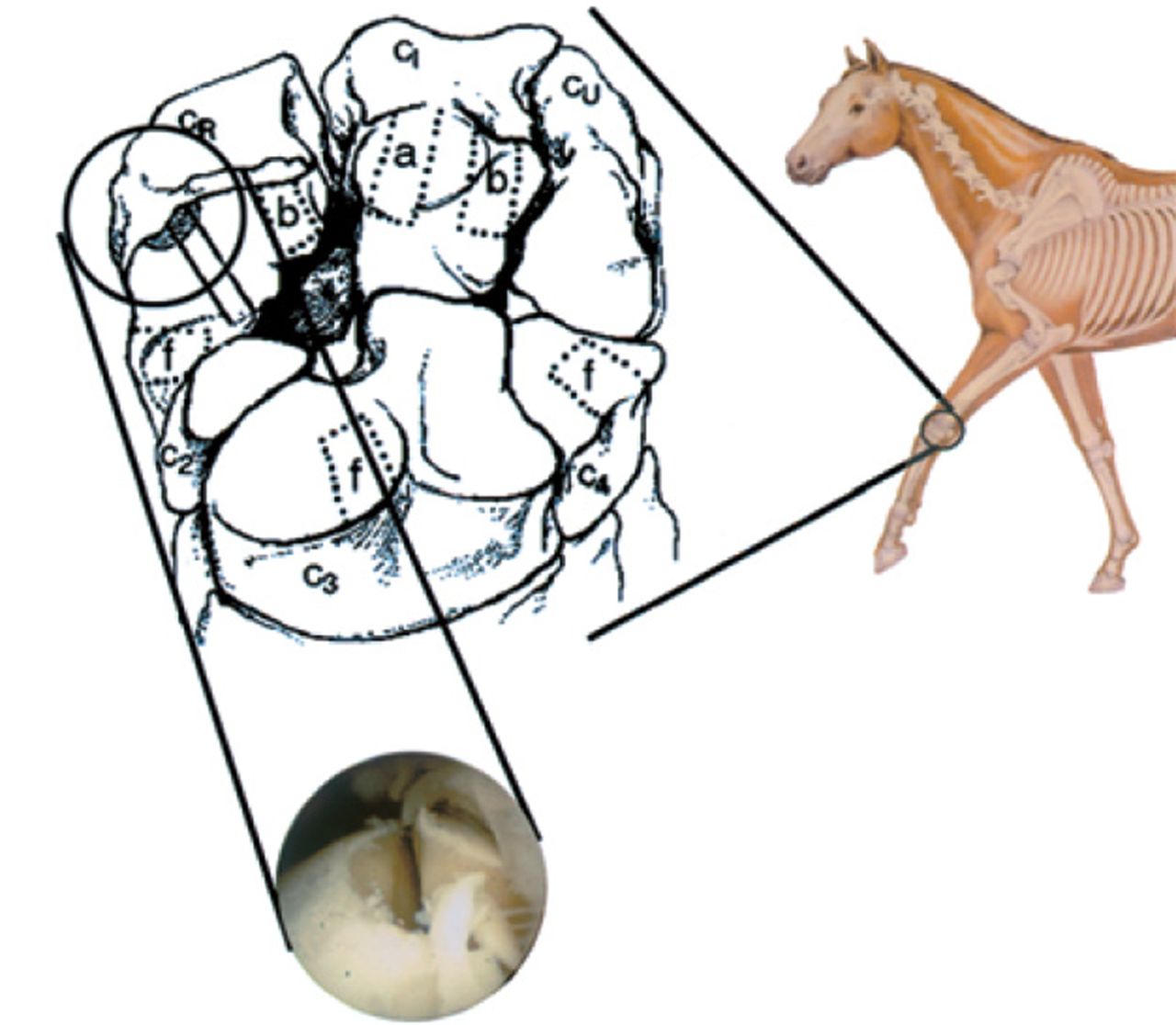
Fig. 5
Image showing the dorsal view of the equine middle carpal joint depicting areas of specific tissue sampling and the osteochondral fragment: a) an area from which articular cartilage was harvested for estimation of proteoglycan synthesis, b) areas from which articular cartilage was harvested for analysis of glycosaminoglycan content, and f) areas from which articular cartilage was harvested for histopathology. The filled in area in the radial carpal bone (CR, circled) represents the osteochondral fragment and the solid lines running through this region represent the section of bone harvested for routine histopathology. The arthroscopic image shows the radial carpal bone after fragment creation and bone debridement (CI, intermediate carpal bone; CU, ulnar carpal bone; C2, second carpal bone; C3, third carpal bone; C4, fourth carpal bone) (reproduced with permission from Frisbie DD et al. Treatment of experimental equine osteoarthritis by in vivo delivery of the equine interleukin-1 receptor antagonist gene. Gene Therapy 2002;9:12–20).
Clinical outcomes
Clinical examination of both forelimbs is performed bi-weekly from pre-surgery throughout the study period, including lameness graded on a scale of 0 to 5 (0 being no lameness and 5 being non-weight bearing lameness)104 and mid-carpal joint effusion graded on a scale of 0 to 4 (0 being no effusion and 4 being the most severe level).50Figure 6 demonstrates the difference between lameness scores and synovial effusion scores between joints treated with IL-1ra gene therapy and placebo.
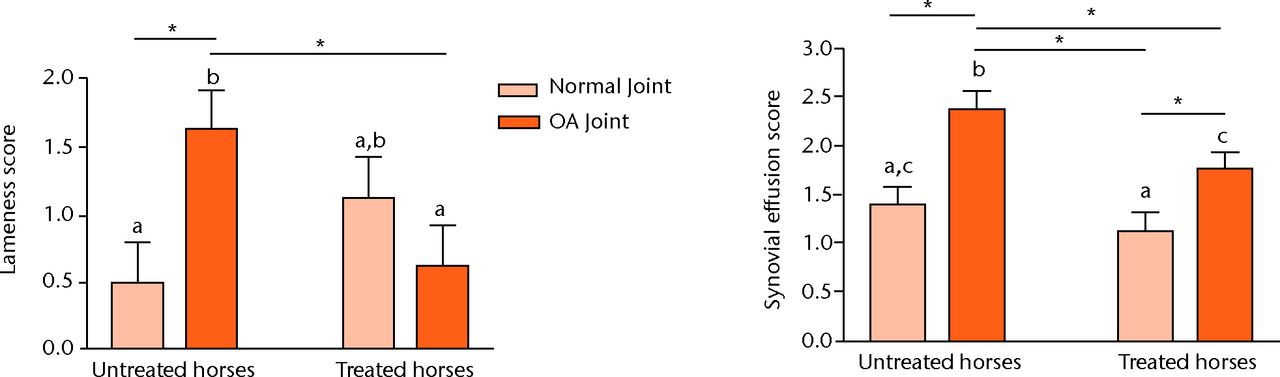
Fig. 6
Bar charts showing the effect of gene transfer 70 days after surgery on lameness score (left) and the synovial effusion score (right). Different letters indicate a statistical difference (p < 0.05) between bars. Alternatively when bars have the same letter, as for example in the untreated and treated normal joints, there is no significant difference between these. Lines with an asterisk (*) linking treatment groups also indicate a statistical difference between treatment groups. Comparisons marked with (*) showing significant differences equate with letters on the bars being different (reproduced with permission from Frisbie DD et al. Treatment of experimental equine osteoarthritis by in vivo delivery of the equine interleukin-1 receptor antagonist gene. Gene Therapy 2002;9:12–20).
Imaging
Radiographs are taken before commencement of the study and at the end of the study. Joints typically show radiological lysis and bony proliferation in the joint capsule attachment within the fibrous joint capsule attachment (enthesophyte). Osteophytosis is also observed. Other imaging modalities have been validated.77 In a comparison of OA-affected carpal joint and normal carpal joints subjected to the exercise protocol a significant increase in nuclear scintigraphic uptake in the OA-affected joints, an increase in the volume of sclerotic bone in the trabecular area of the radial carpal bone with CT and an increase in synovial fluid volume, synovial membrane proliferation, higher joint capsule thickening, joint capsule oedema, radial carpal bone oedema and radial carpal sclerosis on MRI was seen.77
Synovial fluid analysis
Synovial fluid is collected at the time of surgery and at nine additional evenly spaced time periods between surgery and the termination of the study at 70 days. Levels of synovial fluid protein and PGE2 are significantly elevated in OA-affected joints. In a detailed study of biomarkers the levels of CS846, CPII, GAG, ColCEQ, C1,2C, osteocalcin, Col-1 and PGE2 in the OA-affected joints were significantly elevated within 14, seven, 42, 56, 91 and 35 days respectively.76 Serum levels of CS846, CPII, GAG, osteocalcin, C1,2C and Col-1 had a statistically significant increase compared with exercise-alone horses.76
Macroscopic examination
All joints in which OA is induced exhibit some level of pathological change in the form of partial or full-thickness articular cartilage erosions; mostly in a site remote to the osteochondral fragment used to induce the OA. Furthermore, the most pronounced full-thickness erosions are observed independent of ‘kissing’ lesions adjacent to the osteochondral fragment, suggesting that these lesions are a result of OA secondary to the surgery and synovitis. Figure 7 represents a comparison of the macroscopic changes between untreated and AD-Eq IL-1ra treated joints.50 Synovial membrane haemorrhage is also present in affected joints. The macroscopic staging system to describe gross changes in the induced osteochondral chip fragment-exercise OA model has recently been detailed.13
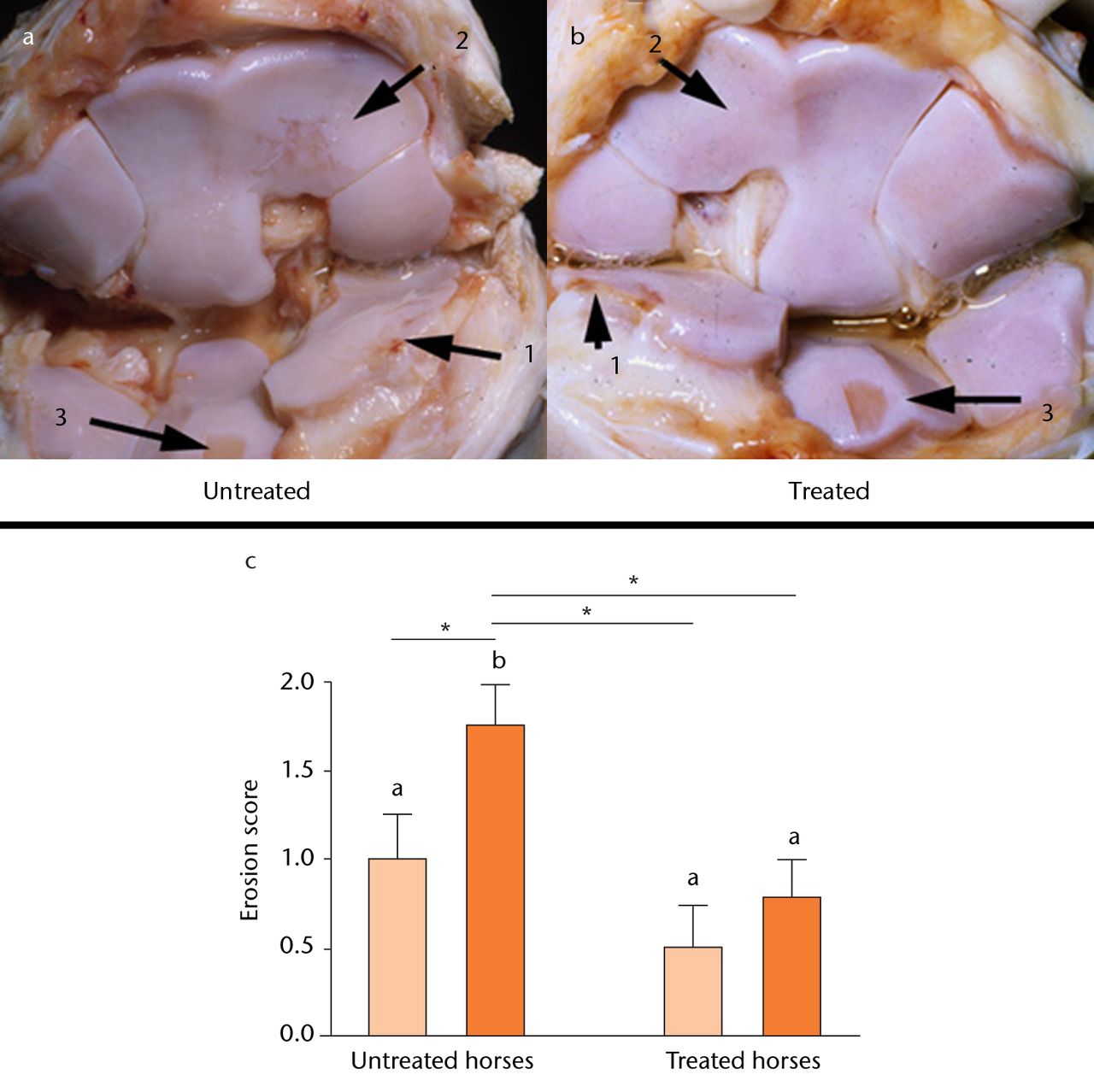
Fig. 7
Diagrams showing the effect of osteoarthritis (OA) and gene transfer on cartilage erosion. Figures 7a and 7b – photographs showing the middle carpal joint highlighting third carpal bone lesions in OA joints of untreated horses (a) and those treated with adenovirus-equine interleukin-1 receptor antagonist (Ad-EqIL-1Ra) (b). Note more extensive full-thickness articular cartilage erosions in the untreated joint (a), especially in areas of the third carpal bone (2) not adjacent to the osteochondral fragment (1). Photos were taken after aseptic harvest of cartilage from the intermediate carpal bone (3). Figure 7c – bar chart showing cartilage erosion scores by treatment group. Different letters associated with bars indicate a statistical difference (p < 0.05) between bars. Lines with an asterisk (*) linking treatment groups also indicate a statistical difference between treatment groups. For instance, there is no difference between untreated and treated normal joints, but a significant difference between untreated and treated OA joints (reproduced with permission from Frisbie DD et al. Treatment of experimental equine osteoarthritis by in vivo delivery of the equine interleukin-1 receptor antagonist gene. Gene Therapy 2002;9:12–20).
Histologic evaluation of synovial membrane
In this model, OA is accompanied by a mild synovitis. There is an increase in cellular infiltration primarily characterised by perivascular lymphocytic infiltration as well as intimal hyperplasia and subintimal oedema.50 The microscopic grading system for synovial membrane histology in the carpal osteochondral fragment model has recently been detailed as part of the OARSI histopathology initiative.13
Histological and histochemical evaluation of articular cartilage
Five micron articular cartilage sections are evaluated from three different locations within each joint for fibrillation, chondrocyte necrosis, chondrocyte cluster formation (previously called chondrone formation) and focal cell loss. Similar results are seen with each location so the results are totalled for all sections. Typically there is an increase in fibrillation and chondrocyte cluster formation. The articular sections stained with Safranin-O and fast green (SOFG) are also evaluated in three different locations within the joints and the OA reduces the SOFG score (Fig. 8). A microscopic grading system for articular cartilage histology has recently been detailed.13
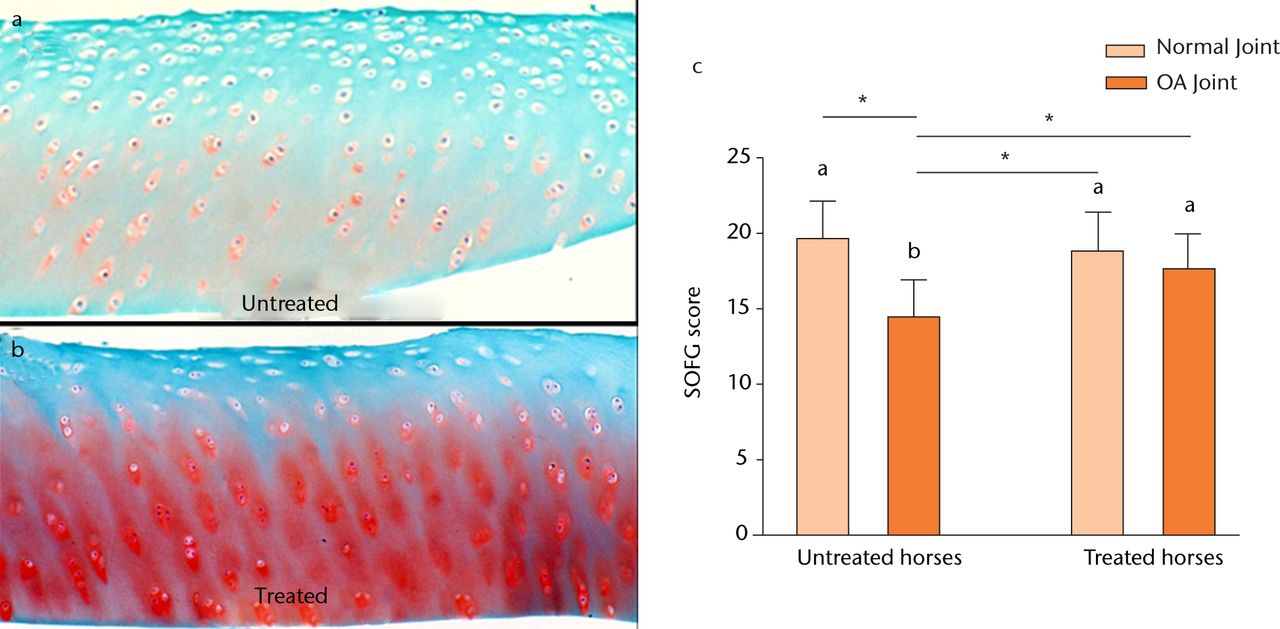
Fig. 8
Diagrams showing the effect of osteoarthritis (OA) and gene transfer on cartilage histology. Figures 8a and 8b – photomicrographs from 5 µm sections of OA articular cartilage stained with Safranin-O and fast green (SOFG) in a) an OA joint of an untreated horse, showing little or no stain uptake in all areas, and b) an OA joint of a horse treated with Ad-EqIL-1ra, showing moderate stain uptake patterns in all areas. Figure 8c – bar chart showing the effect of OA and gene transfer on cartilage staining scores. Different letters associated with bars indicate a statistical difference (p < 0.05) between bars. Lines with an asterisk (*) linking treatment groups also indicate a statistical difference between treatment groups. For instance, there is no difference between untreated and treated normal joints, but a significant difference between untreated and treated OA joints (reproduced with permission from Frisbie DD et al. Treatment of experimental equine osteoarthritis by in vivo delivery of the equine interleukin-1 receptor antagonist gene. Gene Therapy 2002;9:12–20).
Cartilage matrix content and cartilage matrix synthesis
Articular cartilage is harvested from one location to evaluate proteoglycan synthesis at day 70 after surgery using 35SO4 incorporation and total GAG content is measured with the dimethyl methylene blue dye binding assay.
Evaluation of OA treatments with osteochondral fragment-exercise model
The following are summaries of evaluation of various pharmacological and biological treatments performed with this model.
Intra-articular corticosteroids
The use of intra-articular corticosteroids for equine joint disease treatment has long been controversial, but controlled studies with this model have allowed clarification of beneficial versus harmful effects.106 Three corticosteroids commonly used in equine sports medicine have been evaluated. The first product studied was betamethasone esters (Celestone Soluspan; Schering-Plough (now Merck), Whitehouse Station, New Jersey). Treated joints received 2.5 ml of Celestone Soluspan at 14 days after surgery and this was repeated at 35 days, with control joints being injected with saline. No deleterious, adverse effects in the articular cartilage were demonstrated. Two other studies evaluated methylprednisolone acetate (MPA) (Depo Medrol; Pfizer Animal Health, New York, New York) (100 mg at 14 and 28 days) and triamcinolone acetonide (TA) (Vetalog (Fort Dodge Animal Health, Fort Dodge, Iowa) or Kenalog (Bristol-Myers Squibb, Princeton, New Jersey) (12 mg at 14 and 28 days). In OA joints treated with MPA there were positive SMOAD effects, but the modified Mankin scores13 (the score for histopathologicical change in the articular cartilage) were notably increased suggesting deleterious effects of intra-articular administration of MA and negative DMOAD effects. This was in contrast to the results with TA, where horses that were injected IA with TA in OA joints had both significant SMOAD as well as DMOAD effects. The results overall supported favourable effects of TA on degree of clinically detectable lameness, synovial fluid, synovial membrane and articular cartilage morphological parameters both with direct IA administration.
Hyaluronan (HA)
In a recent controlled study with intra-articular HA, the treated joint received 20 mg of HA (Hyvisc; Boehringer Ingelhelm, Ridgefield, Connecticut) at 14, 21 and 28 days. There was a trend for (p < 0.1) for decreased vascularity and subintimal fibrosis but significantly less articular cartilage fibrillation with HA at day 70 (p < 0.05) confirming the drug’s efficacy as a disease-modifying osteo-arthritic drug (DMOAD).107 Intra-articular HA and triamcinolone acetonide are commonly injected together for traumatic arthritis and OA in horses, and it could be rationalised that the triamcinolone acetonide provides an immediate and potent anti-inflammatory effect with long-term DMOAD benefits from the HA.
Intra-articular polysulfated glycosaminoglycan (PSGAG)
This was used for human OA in previous times in Germany but this practice has been discontinued. Treatment with PSGAG (Adequan, 250 mg; Luitpold Animal Health, Shirley, New York) at 14, 21, and 28 days showed significantly decreased synovial effusion with PSGAG compared with placebo (saline) as well as significantly reduced synovial membrane vascularity and subintimal fibrosis. There was a trend for less cartilage fibrillation with PSGAG, so it was concluded that the product had symptom-modifying osteo-arthritic drug (SMOAD) properties as well as DMOAD properties.107 This drug is a common treatment in clinical equine OA.
Gene therapy with intra-articular equine IL-1 receptor antagonist gene
Examples from this study have been given previously. The summary of this project is that IL-1ra gene transferred with an adenoviral vector had the most potent SMOAD and DMOAD effects of any product tested in our osteochondral fragment model of OA with a single injection resulting in significant improvement in clinical parameters of pain and disease activity (Fig. 6), preservation of articular cartilage (Fig. 7) and beneficial effects on the histologic parameters of synovial membrane and articular cartilage (Fig. 8).50 Because of the adenoviral vector used re-dosing was not possible but work has continued in developing a more effective aav vector108 that is currently in dose titration studies with plans to test in our equine OA model.
Autologous conditioned serum
The use of autologous conditioned serum (ACS) (Orthokine; Orthogen Veterinary GmbH, Dussoldorf, Germany) on humans has been previously reported.109 It was considered to have its main effect through upregulation of the expression of several beneficial cytokines including IL-1ra. ACS (6 ml) was injected into equine OA-affected joints on days 14, 21, 28 and 35 respectively, with 6 ml saline administered to the control joints.96 Horses that were treated with ACS had significant clinical improvement in lameness and significantly decreased synovial membrane hyperplasia compared with placebo treated joints, and there also was a trend for less gross cartilage fibrillation. Recently, clinical benefits for persistent knee effusion in people have been demonstrated with the use of the IL-1ra anakinra (Kineret; Amgen, Thousand Oaks, California). Patients refractory to other modalities showed 66% (four of six) improvement in knee arc of motion, 83% (five of six) improvement in pain and 83% (five of six) had improvement in swelling. All of the patients were able to return to sport.110
Evaluation of bone marrow-derived mesenchymal stem cells and adipose-derived stromal vascular fraction
Single intra-articular injections of adipose-derived stromal vascular fraction (SVF) or bone marrow-derived mesenchymal stem cells(BMSCs) (separate groups) were tested in the equine OA model. The only significant change was a greater improvement in synovial fluid PGE2 levels with BMSCs compared with placebo and SVF. Overall the findings of this study were not significant enough to recommend the use of stem cells for the treatment of OA as represented in this model.111
Intramuscular pentosan polysulfate
In a study testing intramuscular pentosan polysulfate (NaPPS 3 mg/kg IM) on study days 15, 22, 29 and 36, articular cartilage fibrillation was substantially reduced by NaPPS treatment. Concentrations of chondroitin sulphate 846 epitope (a synthetic biomarker) were significantly increased in the synovial fluid of osteo-arthritic and non-osteo-arthritic joints of treated horses.112 The conclusion was that NaPPS had some beneficial DMOAD effects and is enjoying increased use for clinical OA in horses.
Other studies
The model has also been used to show beneficial effects of topically administered diclofenac liposomal cream,113 intravenous hyaluronan,47 oral avocado and soy bean unsaponifiable extract,97 extracorporeal shockwave treatment,114 as well as improvement in serum and synovial fluid biomarkers of cartilage and bone with extracorporeal shockwave therapy.115
Articular cartilage defects as part of the OA syndrome: equine studies
While details of repair of articular cartilage defects are beyond the scope of this paper they should be acknowledged as being part of the OA syndrome. It has been shown that even asymptomatic cartilage lesions double the rate of cartilage loss in comparison with intact knees and approximately 80% of lesions progress in size.116,117 Equine chondral defect models have been recently recognised to have specific advantages for translation to human articular cartilage regeneration and have recently been reviewed.118 An equine medial femoral condyle defect model has been used to study subchondral microfracture,119-121 augmentive gene therapy59 and intra-articular BMSC treatment.122 Femoral trochlear defects have been used to evaluate autologous chondrocyte implantation (ACI)123 and the autologous cartilage fragment-loaded scaffold (CAIS) technique.124
1 Anderson DD , ChubinskayaS, GuilakF, et al.Post-traumatic osteoarthritis: improving understanding and opportunities for early intervention. J Orthop Res2011;29:802–809. Google Scholar
2 Goldring MB , GoldringSR. Osteoarthritis. J Cell Physiol2007;213:626–634.CrossrefPubMed Google Scholar
3 Loeser RF . Age-related changes in the musculoskeletal system and the development of osteoarthritis. Clin Geriatr Med2010;26:371–386.CrossrefPubMed Google Scholar
4 Lawrence RC , FelsonDT, HelmickCG, et al.Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum2008;58:26–35.CrossrefPubMed Google Scholar
5 Altman RD , AbramsonS, BruyereO, et al.Commentary: osteoarthritis of the knee and glucosamine. Osteoarthritis Cartilage2006;14:963–966.CrossrefPubMed Google Scholar
6 Saltzman CL , ZimmermanMB, O’RourkeM, et al.Impact of comorbidities on the measurement of health in patients with ankle osteoarthritis. J Bone Joint Surg [Am]2006;88-A:2366–2372.CrossrefPubMed Google Scholar
7 Dirschl DR , MarshJL, BuckwalterJA, et al.Articular fractures. J Am Acad Orthop Surg2004;12:416–423. Google Scholar
8 Gelber AC , HochbergMC, MeadLA, et al.Joint injury in young adults and risk for subsequent knee and hip osteoarthritis. Ann Intern Med2000;133:321–328.CrossrefPubMed Google Scholar
9 Gillquist J , MessnerK. Anterior cruciate ligament reconstruction and the long-term incidence of gonarthrosis. Sports Med1999;27:143–156.CrossrefPubMed Google Scholar
10 Roos H , LaurénM, AdalberthT, et al.Knee osteoarthritis after meniscectomy: prevalence of radiographic changes after twenty-one years, compared with matched controls. Arthritis Rheum1998;41:687–693.CrossrefPubMed Google Scholar
11 Weigel DP , MarshJL. High-energy fractures of the tibial plateau: knee function after longer follow-up. J Bone Joint Surg [Am]2002;84-A:1541–1551. Google Scholar
12 McIlwraith CW . Frank Milne Lecture: From arthroscopy to gene therapy: 30 years of looking in joints. Am Assoc Equine Pract2005;51:65–113. Google Scholar
13 McIlwraith CW , FrisbieDD, KawcakCE, et al.The OARSI histopathology initiative: recommendations for histological assessments of osteoarthritis in the horse. Osteoarthritis Cartilage2010;18(Suppl 3):S93–S105. Google Scholar
14 McIlwraith CW. General pathobiology of the joint and response to injury. In: McIlwraith CW, Trotter GW, eds. Joint disease in the horse. Philadelphia: WB Saunders Company, 1996:40–70. Google Scholar
15 Goodrich LR , NixonAJ. Medical treatment of osteoarthritis in the horse: a review. Vet J2006;171:51–69. Google Scholar
16 Caron JP. Osteoarthritis. In: Ross MW, Dyson SJ, eds. Diagnosis and management of lameness in the horse. 2nd edition. St Louis: Elsevier Saunders, 2011:655–668. Google Scholar
17 United States Department of Agriculture. Lameness and laminitis in U.S. Horses. National Animal Health Monitoring System, 2000. http://www.aphis.usda.gov/animal_health/nahms/equine/downloads/equine98/Equine98_dr_Lameness.pdf (date last accessed 20 September 2012). Google Scholar
18 Caron JP, Genovese RL. Principles and practices of joint disease treatment. In: Ross MW, Dyson SJ, eds. Diagnosis and management of lameness in the horse. Philadelphia: Elsevier, 2003:746–764. Google Scholar
19 Koch TG , BettsDH. Stem cell therapy for joint problems using the horse as a clinically relevant animal model. Expert Opin Biol Ther2007;7:1621–1626.CrossrefPubMed Google Scholar
20 Pritzker KP , GayS, JimenezSA, et al.Osteoarthritis cartilage histopathology: grading and staging. Osteoarthritis Cartilage2006;14:13–29.CrossrefPubMed Google Scholar
21 Dray A , ReadSJ. Arthritis and pain: future targets to control osteoarthritis pain. Arthritis Res Ther2007;9:212. Google Scholar
22 Neundorf RH , LowerisonMB, CruzAM, et al.Determination of the prevalence and severity of metacarpophalangeal joint osteoarthritis in Thoroughbred racehorses via quantitative macroscopic evaluation. Am J Vet Res2010;71:1284–1293.CrossrefPubMed Google Scholar
23 Norrdin RW , StoverSM. Subchondral bone failure in overload arthrosis: a scanning electron microscopic study in horses. J Musculoskelet Neuronal Interact2006;6:251–257.PubMed Google Scholar
24 Drum MG , KawcakCE, NorrdinRW, et al.Comparison of gross and histopathologic findings with quantitative computed tomographic bone density in the distal third metacarpal bone of racehorses. Vet Radiol Ultrasound2007;48:518–527.CrossrefPubMed Google Scholar
25 Callender GR , KelserRA. Degenerative arthritis: a comparison of the pathological changes in man and equines. Am J Pathol1938;38:253–272.PubMed Google Scholar
26 Mackay-Smith MP . Pathogenesis and pathology of equine osteoarthritis. J Am Med Vet Assoc1962;141:1246–1252. Google Scholar
27 Raker CW , BakerRH, WheatJD. Pathophysiology of equine degenerative joint disease and lameness. Am Assoc Equine Pract1966;12:229–241. Google Scholar
28 Rooney JR. Biomechanics of lameness in horses. Baltimore: Williams and Wilkins, 1969. Google Scholar
29 Nilsson G , OlssonSC. Radiologic and patho-anatomical changes in the distal joints and phalanges of the standardbred horse. Acta Vet Scand Suppl1973;44:1–57. Google Scholar
30 Brandt KD , DieppeP, RadinEL. Etiopathogenesis of osteoarthritis. Rheum Dis Clin North Am2008;34:531–559.CrossrefPubMed Google Scholar
31 McIlwraith CW . Current concepts in equine degenerative joint disease. J Am Vet Med Assoc1982;180:239–250.PubMed Google Scholar
32 Riggs CM , WhitehouseGH, BoydeA. Pathology of the distal condyles of the third metacarpal and third metatarsal bones of the horse. Equine Vet J1999;31:140–148.CrossrefPubMed Google Scholar
33 Kawcak CE , McIlwraithCW, NorrdinRW, ParkRD, JamesSP. The role of subchondral bone in joint disease: a review. Equine Vet J2001;33:120–126.CrossrefPubMed Google Scholar
34 McIlwraith CW , YovichJV, MartinGS. Arthroscopic surgery for the treatment of osteochondral chip fractures in the equine carpus. J Am Vet Med Assoc1987;191:531–540.PubMed Google Scholar
35 Kawcak CE , McIlwraithCW. Proximodorsal first phalanx osteochondral chip fragmentation in 336 horses. Equine Vet J1994;26:392–396.CrossrefPubMed Google Scholar
36 Frisbie DD , RayCS, IonescuM, et al.Measurement of synovial fluid and serum concentrations of the 846 epitope of chondroitin sulfate and of carboxy propeptides of type II procollagen for diagnosis of osteochondral fragmentation in horses. Am J Vet Res1999;60:306–309.PubMed Google Scholar
37 Fuller CJ , BarrAR, SharifM, DieppePA. Cross-sectional comparison of synovial fluid biochemical markers in equine osteoarthritis and the correlation of these markers with articular cartilage damage. Osteoarthritis Cartilage2001;9:49–55.CrossrefPubMed Google Scholar
38 McIlwraith CW , VachonA. Review of pathogenesis and treatment of degenerative joint disease. Equine Vet J Suppl1988;6:3–11.CrossrefPubMed Google Scholar
39 Buckwalter JA . Articular cartilage injuries. Clin Orthop Relat Res2002;402:21–37.CrossrefPubMed Google Scholar
40 Buckwalter JA , BrownTD. Joint injury, repair, and remodelling: roles in post-traumatic osteoarthritis. Clin Orthop Relat Res2004;423:7–16. Google Scholar
41 Olson SA , GuilakF. From articular fracture to posttraumatic arthritis: a black box that needs to be opened. J Orthop Trauma2006;20:661–662.CrossrefPubMed Google Scholar
42 McIlwraith CW , Van SickleDC. Experimentally induced arthritis of the equine carpus: histologic and histochemical changes in the articular cartilage. Am J Vet Res1981;42:209–217.PubMed Google Scholar
43 Balkman CE , NixonAJ. Molecular cloning and cartilage gene expression of equine stromelysin 1 (matrix metalloproteinase 3). Am J Vet Res1998;59:30–36.PubMed Google Scholar
44 Clegg PD , BurkeRM, CoughlanAR, RiggsCM, CarterSD. Characterisation of equine matrix metalloproteinase 2 and 9; and identification of the cellular sources of these enzymes in joints. :. Equine Vet J1997;29:335–342. Google Scholar
45 Clegg PD , CoughlanAR, RiggsCM, CarterSD. Matrix metalloproteinases 2 and 9 in equine synovial fluids. Equine Vet J1997;29:343–348.CrossrefPubMed Google Scholar
46 Trumble TN , TrotterGW, OxfordJR, et al.Synovial fluid gelatinase concentrations and matrix metalloproteinase and cytokine expression in naturally occurring joint disease in horses. Am J Vet Res2001;62:1467–1477.CrossrefPubMed Google Scholar
47 Kawcak CE , FrisbieDD, TrotterGW, et al.Effects of intravenous administration of sodium hyaluronate on carpal joints in exercising horses after arthroscopic surgery and osteochondral fragmentation. Am J Vet Res1997;58:1132–1140.PubMed Google Scholar
48 Dimock AN , SicilianoPD, McIlwraithCW. Evidence supporting an increased presence of reactive oxygen species in the diseased equine joint. Equine Vet J2000;32:439–443.CrossrefPubMed Google Scholar
49 Takafuji VA , McIlwraithCW, HowardRD. Effects of recombinant equine interleukin-1 alpha and interleukin-1 beta on proteoglycan metabolism and prostaglandin E2 synthesis in equine articular cartilage explants. Am J Vet Res2002;63:551–558. Google Scholar
50 Frisbie DD , GhivizzaniSC, RobbinsPD, EvansCH, McIlwraithCW. Treatment of experimental equine osteoarthritis by in vivo delivery of the equine interleukin-1 receptor antagonist gene. Gene Ther2002;9:12–20.CrossrefPubMed Google Scholar
51 Kamm JL , NixonAJ, WitteTH. Cytokine and catabolic enzyme expression in synovium, synovial fluid and articular cartilage of naturally osteoarthritic equine carpi. Equine Vet J2010;42:693–699.CrossrefPubMed Google Scholar
52 Frisbie DD , McIlwraithCW. Gene therapy: future therapies in osteoarthritis. Vet Clin North Am Equine Pract2001;17:233–243.CrossrefPubMed Google Scholar
53 Berenbaum F . The quest for the Holy Grail: a disease-modifying osteoarthritis drug. Arthritis Res Ther2007;9:111.CrossrefPubMed Google Scholar
54 Toncheva A , RemichkovaM, IkonomovaK, DimitrovaP, IvanovskaN. Inflammatory response in patients with active and inactive osteoarthritis. Rheumatol Int2009;29:1197–1203.CrossrefPubMed Google Scholar
55 Wassilew GI , LehnigkU, DudaGN, et al.The expression of proinflammatory cytokines in matrix metalloproteinases in the synovial membranes of patients with osteoarthritis compared with traumatic knee disorders. Arthroscopy2010;26:1096–1104. Google Scholar
56 Goekoop RJ , KloppenburgM, KroonHM, et al.Low innate production of interleukin-1beta and interleukin-6 is associated with the absence of osteoarthritis in old age. Osteoarthritis Cartilage2010;18:942–947.CrossrefPubMed Google Scholar
57 Sellam J , BernbaumF. The role of synovitis in pathophysiology and clinical symptoms of osteoarthritis. Nature Rev Rheum2010;6:625–635.CrossrefPubMed Google Scholar
58 Mueller MB , TuanRS. Anabolic/catabolic balance in pathogenesis of osteoarthritis: identifying molecular targets. PM R2011;3(Suppl):S3–S11.CrossrefPubMed Google Scholar
59 Morisset S , FrisbieDD, RobbinsPD, NixonAJ, McIlwraithCW. IL-1ra/IGF-1 gene therapy modulates repair of microfractured chondral defects. Clin Orthop Relat Res2007;462:221–228.CrossrefPubMed Google Scholar
60 Varich L , PathriaM, ResnickD, et al.Patterns of central acetabular osteophytosis and osteoarthritis of the hip. Invest Radiol1993;28:1120–1127. Google Scholar
61 McCauley TR . MR imaging of chondral and osteochondral injuries of the knee. Radiol Clin North Am2002;40:1095–1107.CrossrefPubMed Google Scholar
62 Olive J , D’AnjouMA, GirardC, LavertyS, TheoretCL. Imaging and histological features of central subchondral osteophytes in racehorses with metacarpophalangeal joint osteoarthritis. Equine Vet J2009;41:859–864.CrossrefPubMed Google Scholar
63 Steinmeyer J , KonttinenYT. Oral treatment options for degenerative joint disease: present and future. Adv Drug Deliv Rev2006;58:168–211. Google Scholar
64 Zhang W , DohertyM, ArdenB, et al.EULAR evidence based recommendations for the management of hip osteoarthritis: report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis2005;64:669–681.CrossrefPubMed Google Scholar
65 Jordan KM , ArdenNK, DohertyM, et al.EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis2003;62:1145–1155.CrossrefPubMed Google Scholar
66 No authors listed. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update: American College of Rheumatology Subcommittee on Osteoarthritis Guidelines Arthritis Rheum2000;43:1905–1915. Google Scholar
67 Chard JA , TallonD, DieppePA. Epidemiology of research into interventions for the treatment of osteoarthritis of the knee joint. Ann Rheum Dis2000;59:414–418.CrossrefPubMed Google Scholar
68 McAlindon TE , LaValleyMP, GulinJP, FelsonDT. Glucosamine and chondroitin for treatment of osteoarthritis: a systematic quality assessment and meta-analysis. J Am Med Assoc2000;283:1469–1475.CrossrefPubMed Google Scholar
69 Qvist P , Bay-JensenAC, ChristiansenC, et al.The disease modifying osteoarthritic drug (DMOAD): is it in the horizon?Pharmacol Res2008;58:1–7. Google Scholar
70 Bingham CO , Buckland-WrightJC, GarneroP, et al.Risedronate decreases biochemical markers of cartilage degradation but does not decrease symptoms or slow radiographic progression in patients with medial compartment osteoarthritis of the knee: results of the two-year multinational knee osteoarthritis structural arthritis study. Arthritis Rheum2006;54:3494–3507.CrossrefPubMed Google Scholar
71 Gaustad G , LarsenS. Comparison of polysulfated glycosaminoglycan and sodium hyaluronate with placebo and treatment of traumatic arthritis in horses. Equine Vet J1995;27:356–362. Google Scholar
72 Sabaté D , HomedesJ, SalichsM, SustM, MonrealL. Multicentre, controlled, randomised and blinded field study comparing efficacy of suxibuzone and phenylbutazone in lame horses. Equine Vet J2009;41:700–705.CrossrefPubMed Google Scholar
73 Gough MR , ThibaudD, SmithRK. Tiludronate infusion in the treatment of bone spavin: a double blind, placebo-controlled trial. Equine Vet J2010;42:381–387. Google Scholar
74 Cayzer J , HedderleyD, GrayS. A randomized, double-blinded, placebo-controlled study on the efficacy of a unique extract of green-lip mussel (Perna canaliculus) in horses with chronic fetlock lameness attributed to osteoarthritis. Equine Vet J2012;44:393–398. Google Scholar
75 Clegg PD . Investigating the efficacy of articular medications in the horse: the science behind clinical practices. Equine Vet J2010;42:484–486.CrossrefPubMed Google Scholar
76 Frisbie DD , Al-SobayilF, BillinghurstRC, KawcakCE, McIlwraithCW. Changes in synovial fluid and serum biomarkers with exercise and early osteoarthritis in horses. Osteoarthritis Cartilage2008;16:1196–1204.CrossrefPubMed Google Scholar
77 Kawcak CE , FrisbieDD, WerpyNM, ParkRD, McIlwraithCW. Effects of exercise vs experimental osteoarthritis on imaging outcomes. Osteoarthritis Cartilage2008;16:1519–1525.CrossrefPubMed Google Scholar
78 Le Graverand-Gastineau MP . Disease modifying osteoarthritic drugs: facing development challenges in choosing molecular targets. Curr Drug Targets2010;11:528–535. Google Scholar
79 Aigner T , CookJL, GerwinN, et al.Histopathology atlas of animal model systems: overview of guiding principles. Osteoarthritis Cartilage2010;18(Suppl 3):S2–S6. Google Scholar
80 McIlwraith CW , FesslerJF, BlevinsWE, et al.Experimentally induced arthritis of the equine carpus: clinical determinations. Am J Vet Res1979;40:11–20.PubMed Google Scholar
81 Gustafson SB , TrotterGW, NorrdinRW, WrigleyRH, LamarC. Evaluation of intra-articularly administered sodium monoiodoacetate-induced chemical injury to articular cartilage of horses. Am J Vet Res1992;53:1193–1202.PubMed Google Scholar
82 Yovich JV , TrotterGW, McIlwraithCW, NorrdinRW. Effects of polysulfated glycosaminoglycan on chemical and physical defects in equine articular cartilage. Am J Vet Res1987;48:1407–1414.PubMed Google Scholar
83 Trotter GW , YovichJV, McIlwraithCW, NorrdinRW. Effects of intramuscular polysulfated glycosaminoglycan on chemical and physical defects in equine articular cartilage. Can J Vet Res1989;53:224–230.PubMed Google Scholar
84 Peloso JG , StickJA, CaronJP, PelosoPM, Soutas-LittleRW. Effects of hylan on amphotericin-induced carpal lameness in equids. Am J Vet Res1993;54:1527–1534.PubMed Google Scholar
85 Firth EC , WensingT, SeurenF. An induced synovitis model in ponies. Cornell Vet1987;77:107–118. Google Scholar
86 Todhunter PG , KincaidSA, TodhunterRJ, et al.Immunohistochemical analysis of an equine model of synovitis-induced arthritis. Am J Vet Res1996;57:1080–1093.PubMed Google Scholar
87 Palmer JL , BertoneAL, MalemudCJ, MansourJ. Biochemical and biomechanical alterations in equine articular cartilage following an experimentally-induced synovitis. Osteoarthritis Cartilage1996;4:127–137.CrossrefPubMed Google Scholar
88 Hardy J , BertoneAL, WeisbrodeSE, et al.Cell trafficking, mediator release, and articular metabolism in acute inflammation of innervated or denervated isolated equine joints. Am J Vet Res1998;59:88–100.PubMed Google Scholar
89 Cornelissen BP , RijkenhuizenAB, van den HoogenBM, RuttenVP, BarneveldA. Experimental model of synovitis/capsulitis in the equine metacarpophalangeal joint. Am J Vet Res1998;59:978–985.PubMed Google Scholar
90 Owens JG , KamerlingSG, StantonSR, KeowenML, Prescott-MathewsJS. Effects of pretreatment with ketoprofen and phenylbutazone on experimentally induced synovitis in horses. Am J Vet Res1996;57:866–874.PubMed Google Scholar
91 Auer JA , FackelmanGE, GingerichDA, FetterAW. Effect of hyaluronic acid in naturally occurring and experimentally induced osteoarthritis. Am J Vet Res1980;41:568–574.PubMed Google Scholar
92 Simmons EJ , BertoneAL, WeisbrodeSE. Instability-induced osteoarthritis in the metacarpophalangeal joint of horses. Am J Vet Res1999;60:7–13.PubMed Google Scholar
93 Frisbie DD , KawcakCE, TrotterGW, et al.Effects of triamcinolone acetonide on an in vivo equine osteochondral fragment exercise model. Equine Vet J1997;29:349–359.CrossrefPubMed Google Scholar
94 Kawcak CE , NorrdinRW, FrisbieDD, TrotterGW, McIlwraithCW. Effects of osteochondral fragmentation and intra-articular triamcinolone acetonide treatment on subchondral bone in the equine carpus. Equine Vet J1998;30:66–71.CrossrefPubMed Google Scholar
95 Frisbie DD , KawcakCE, BaxterGM, et al.Effects of 6-alpha-methylprednisolone acetate on an equine osteochondral fragment exercise model. Am J Vet Res1998;59:1619–1628. Google Scholar
96 Frisbie DD , KawcakCE, WerpyNM, ParkRD, McIlwraithCW. Clinical, biochemical and histologic effects of intra-articular administration of autologous conditioned serum in horses with experimentally induced osteoarthritis. Am J Vet Res2007;68:290–296. Google Scholar
97 Kawcak CE , FrisbieDD, McIlwraithCW, WerpyNM, ParkRD. Evaluation of avocado and soybean unsaponifiable extracts for treatment of horses with experimentally induced osteoarthritis. Am J Vet Res2007;68:598–604.CrossrefPubMed Google Scholar
98 Bolam CJ , HurtigMB, CruzA, McEwenBJ. Characterization of experimentally induced post-traumatic osteoarthritis in the medial femorotibial joint of horses. Am J Vet Res2006;67:433–447.CrossrefPubMed Google Scholar
99 Frisbie DD , CrossMW, McIlwraithCW. A comparative study of articular cartilage thickness in the stifle of animal species used in human pre-clinical studies compared to articular cartilage thickness in the human knee. Vet Comp Orthop Traumatol2006;19:142–146.PubMed Google Scholar
100 Richardson DW , ClarkCC. Effects of short-term cast immobilization on equine articular cartilage. Am J Vet Res1993;54:449–453.PubMed Google Scholar
101 van Harreveld PD , LillichJD, KawcakCE, et al.Clinical evaluation of the effects of immobilization followed by remobilization and exercise on the metacarpophalangeal joint in horses. Am J Vet Res2002;63:282–288.CrossrefPubMed Google Scholar
102 van Harreveld PD , LillichJD, KawcakCE, TurnerAS, NorrdinRW. Effects of immobilization followed by remobilization on mineral density, histomorphometric features, and formation of the bones of the metacarpophalangeal joint in horses. Am J Vet Res2002;63:276–281.CrossrefPubMed Google Scholar
103 Foland JW , McIlwraithCW, TrotterGW, PowersBE, LamarCH. Effect of betamethasone and exercise on equine carpal joints with osteochondral fragments. Vet Surg1994;23:369–376.CrossrefPubMed Google Scholar
104 No authors listed. Definition and classification of lameness. In: Guide for veterinary service and judging of equestrian events. Lexington: American Association of Equine Practitioners, 1991:19. Google Scholar
105 Peterson B , SzaboRM. Carpal osteoarthrosis. Hand Clin2006;22:517–528.CrossrefPubMed Google Scholar
106 McIlwraith CW . The use of intra-articular corticosteroids in the horse: what is known on a scientific basis?Equine Vet J2010;42:563–571.CrossrefPubMed Google Scholar
107 Frisbie DD , KawcakCE, McIlwraithCW, WerpyNM. Evaluation of polysulfated glycosaminoglycan or sodium hyaluronan administered intra-articularly for treatment of hoses with experimentally induced osteoarthritis. Am J Vet Res2009;70:203–209. Google Scholar
108 Goodrich LR , ChoiVW, CarboneBAD, McIlwraithCW, SamulskiRJ. Ex vivo serotype-specific transduction of equine joint tissue by self-complementary adeno-associated viral vectors. Hum Gene Ther2009;20:1697–1702.CrossrefPubMed Google Scholar
109 Meijer H , ReineckeJ, BeckerC, TholenG, WehlingP. The production of anti-inflammatory cytokines in whole blood by physico-chemical induction. Inflamm Res2003;52:404–407.CrossrefPubMed Google Scholar
110 Brown C , TothA, MagnussenR. Clinical benefits of intra-articular anakinra for persistent knee effusion. J Knee Surg2011;24:61–65.CrossrefPubMed Google Scholar
111 Frisbie DD , KisidayJD, KawcakCE, WerpyNM, McIlwraithCW. Evaluation of adipose-derived stromal vascular fraction or bone marrow-derived mesenchymal stem cells for treatment of osteoarthritis. J Orthop Res2009;27:1675–1680.CrossrefPubMed Google Scholar
112 McIlwraith CW , FrisbieDD, KawcakCE. Evaluation of intramuscularly administered sodium pentosan polysulfate for treatment of experimentally induced osteoarthritis in horses. Am J Vet Res2012;73:628–633.CrossrefPubMed Google Scholar
113 Frisbie DD , McIlwraithCW, KawcakCE, WerpyNM, PearceGL. Evaluation of topically administered diclofenac liposomal cream for treatment of horses with experimentally induced osteoarthritis. Am J Vet Res2009;70:210–215.CrossrefPubMed Google Scholar
114 Frisbie DD , KawcakCE, McIlwraithCW. Evaluation of the effect of extracorporeal shockwave treatment on experimentally induced osteoarthritis in middle carpal joints of horses. Am J Vet Res2009;70:449–454. Google Scholar
115 Kawcak CE , FrisbieDD, McIlwraithCW. Effects of extracorporeal shock wave therapy and polysulfated glycosaminoglycan treatment on subchondral bone, serum biomarkers, and synovial fluid biomarkers in horses with induced osteoarthritis. Am Vet J Res2011;72:772–779.CrossrefPubMed Google Scholar
116 Cicuttini F , DingC, WlukaA, et al.Association of cartilage defects with loss of knee cartilage in healthy, middle-age adults: a prospective study. Arthritis Rheum2005;52:2033–2039.CrossrefPubMed Google Scholar
117 Davies-Tuck ML , WlukaAE, WangY, et al.The natural history of cartilage defects in people with knee osteoarthritis. Osteoarthritis Cartilage2008;16:337–342.CrossrefPubMed Google Scholar
118 McIlwraith CW , FortierLA, FrisbieDD, NixonAJ. Equine models of articular cartilage repair. Cartilage2011;2:317–326.CrossrefPubMed Google Scholar
119 Frisbie DD , TrotterGW, PowersBE, et al.Arthroscopic subchondral bone plate microfracture technique augments healing of large chondral defects in the radial carpal bone and medial femoral condyles of horses. Vet Surg1999;28:242–255. Google Scholar
120 Frisbie DD , OxfordJT, SouthwoodL, et al.Early events in cartilage repair after subchondral bone microfracture. Clin Orthop Relat Res2003;407:215–227.CrossrefPubMed Google Scholar
121 Frisbie DD , MorissetS, HoCP, et al.Effects of calcified cartilage on healing of chondral defects treated with microfracture in horses. Am J Sports Med2006;34:1824–1831.CrossrefPubMed Google Scholar
122 McIlwraith CW , FrisbieDD, RodkeyWG, et al.Evaluation of intra-articular mesenchymal stem cells to augment healing of microfractured chondral defects. Arthroscopy2011;27:1552–1561.CrossrefPubMed Google Scholar
123 Frisbie DD , BowmanSM, ColhounHA, et al.Evaluation of autologous chondrocyte transplantation via a collagen membrane in equine articular defects: results at 12 and 18 months. Osteoarthritis Cartilage2008;16:667–679.CrossrefPubMed Google Scholar
124 Frisbie DD , LuY, KawcakCE, et al.In vivo evaluation of autologous cartilage fragment-loaded scaffolds implanted into equine articular defects and compared with autologous chondrocyte implantation. Am J Sports Med2009;37(Suppl 1):71S–80S.CrossrefPubMed Google Scholar
Funding statement:
None declared
Author contributions:
C. W. McIlwraith: Writing the paper, Reviewing the final manuscript, Led research
D. D. Frisbie: Reviewing the final manuscript, Led research
C. E. Kawcak: Reviewing the final manuscript, Led research
ICMJE Conflict of Interest:
None declared
©2012 British Editorial Society of Bone and Joint Surgery. This is an open-access article distributed under the terms of the Creative Commons Attributions licence, which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
