




Abstract
Objectives
The effects of disease progression and common tendinopathy treatments on the tissue characteristics of human rotator cuff tendons have not previously been evaluated in detail owing to a lack of suitable sampling techniques. This study evaluated the structural characteristics of torn human supraspinatus tendons across the full disease spectrum, and the short-term effects of subacromial corticosteroid injections (SCIs) and subacromial decompression (SAD) surgery on these structural characteristics.
Methods
Samples were collected inter-operatively from supraspinatus tendons containing small, medium, large and massive full thickness tears (n = 33). Using a novel minimally invasive biopsy technique, paired samples were also collected from supraspinatus tendons containing partial thickness tears either before and seven weeks after subacromial SCI (n = 11), or before and seven weeks after SAD surgery (n = 14). Macroscopically normal subscapularis tendons of older patients (n = 5, mean age = 74.6 years) and supraspinatus tendons of younger patients (n = 16, mean age = 23.3) served as controls. Ultra- and micro-structural characteristics were assessed using atomic force microscopy and polarised light microscopy respectively.
Results
Significant structural differences existed between torn and control groups. Differences were identifiable early in the disease spectrum, and increased with increasing tear size. Neither SCI nor SAD surgery altered the structural properties of partially torn tendons seven weeks after treatment.
Conclusions
These findings may suggest the need for early clinical intervention strategies for torn rotator cuff tendons in order to prevent further degeneration of the tissue as tear size increases. Further work is required to establish the long-term abilities of SCI and SAD to prevent, and even reverse, such degeneration.
Cite this article: Bone Joint Res 2014;3:252–61.
Article focus
This study evaluated the structural characteristics of torn human supraspinatus tendons across the full disease spectrum (partial through to massive full-thickness tears), and the short-term effects of subacromial corticosteroid injections (SCIs) and subacromial decompression (SAD) surgery on these structural characteristics
Key messages
Torn supraspinatus tendons exhibit significantly thinner fibrils, higher proportions of thinner fibres, and shorter crimp lengths compared with control samples.
These structural differences occur early in the disease spectrum, appear to increase as tear size increases, and neither SCI nor SAD surgery significantly alter these structural changes seven weeks post-treatment.
Strengths and limitations
Strengths: For the first time, this study quantitatively evaluates the structural characteristics of human rotator cuff tendons across the full disease spectrum, demonstrating the existence of structural changes much earlier in the disease progression than has previously been possible.
This study provides novel insight into the efficiency of common tendinopathy treatments for arresting and reversing degenerative structural changes in the initial stages of disease
Limitations: Conclusions regarding the efficiency of these treatments is limited by the short timescale of the follow-up sample collection.
Introduction
Chronic tendinopathies are widespread and debilitating; the incidence of shoulder sprains, strains and tears is reportedly 47.3 per 10 000 workers in the USA,1 while approximately 5% of patients visiting rheumatologists are suffering from chronic tendinitis.2 Shoulder pain affects up to 30% of the population and is most commonly caused by disorders of the rotator cuff tendon, ranging from inflammation to full thickness tears of the cuff tendon.3 Given the strong correlation between patient age and the incidence of tendinopathies,4,5 the anticipated levels of the population to be ageing6 are likely to give rise to an increase in rotator cuff tendinopathy in the population in the future. Improved understanding and diagnosis of this tendon disorder is therefore urgently needed to aid clinician decisions.
Observations that the presence of tears is strongly associated with ageing have led to speculation of an association between tendinopathy and tissue degeneration.7,8 A number of differences have been reported to exist between torn rotator cuff tendons compared with control samples, such as elevated levels of lipoid degeneration, increased ratios of collagen type III to type I, increased apoptosis, and altered concentrations of matrix metalloproteinases and tissue inhibitors of matrix metalloproteinases.9-11 Observations that the extent of these changes appears to correlate with increasing tear size suggest that disease progression is associated with increased tissue degeneration.12,13 A progressive relationship between tear size and tissue degeneration could explain the importance of tear size as a determinant of the success of rotator cuff repair surgery and, given the correlation between the structure and mechanical behaviour of the tendon,14 could have important implications for our understanding of rotator cuff tendinopathy. The existence of such a relationship, however, has yet to be proved.
It has been shown that torn rotator cuff tendons exhibit a multitude of biochemical and cellular changes, such as altered mucopolysaccharide profiles and chondroid metaplasia,15-17 decreased mechanical integrity18 and structural changes such as thinner fascicles19 and thinner, less-organised collagen fibres10,20 compared with normal tendons. Detailed investigations into the structural characteristics of torn rotator cuff tendons at different scales of length (i.e. ultra- and micro-structure) and across the full disease spectrum – from partial thickness tears through to massive full-thickness tears – have not been reported owing to issues associated with obtaining human tissue samples in the early stages of disease and of a suitable size in order to carry out a range of analyses.18 The existence of a progressive relationship between tear size and changes in the structural properties of torn tendon tissue, therefore, remains to be conclusively demonstrated.
To reduce the risk of further rupture, tendinopathy treatments should aim to prevent further degeneration of ruptured tissue. Initial treatment for rotator cuff disorders often takes the form of subacromial corticosteroid injections (SCIs). Should such conservative measures fail, patients may then receive subacromial decompression (SAD) surgery in order to reduce the impingement of the acromion on the supraspinatus tendon.21 The efficiency of these treatments for preventing or reversing tissue degeneration is not clear.22,23 While repeated use of steroidal injections is associated with decreased mechanical properties and poor post-operative results,24,25 both interventions have been reported to reduce pain and improve function within one month of intervention.23,26 It might therefore be expected that both treatments would influence the structural properties of torn cuff tendons. However, previous human studies have been restricted to intra-operative sampling of either tissue discarded as part of a routine resection during a tendon repair,13,27 or from the structures surrounding the tendon that are resected at SAD surgery.11 There is no existing research that has quantitatively analysed the in vivo tissue response to current treatment for rotator cuff pathology in these tendons within the shoulder.
Transmission electron microscopy (TEM) is traditionally employed to investigate the ultra-structure of biological tissues.28,29 However, this technique requires glutaraldehyde-fixation of samples, limiting its use for analysis of formalin-fixed samples (a common preservation method employed by clinicians immediately following surgery),30 and restricting further characterisation of the samples with common histological and immunohistochemical techniques.31 Conversely, atomic force microscopy (AFM) provides a wealth of structural and compositional information for formalin-fixed, or even fresh, samples at the ultra-structural level without the need for complex preparation techniques or ultra-thin (< 500 nm) samples.32-36 AFM is therefore a tremendously powerful technique, allowing analysis of ultra-structural changes in surgically-obtained tissues37-40 without restricting additional characterisation at the micro-structural level.41
In the present study, atomic force microscopy (AFM) and polarised light microscopy are employed to characterise the collagen ultra-structure (fibrils)42 and micro-structure (fibres)43 of human rotator cuff tendons respectively. For the first time, these structural properties are characterised across the full disease spectrum – from partial thickness tears, to massive full-thickness tears – as well as pre- and post- SCI and SAD surgery in order to investigate the relationship between rotator cuff tendinopathy, common interventions and the structural properties of cuff tendons. It is hypothesised that torn human supraspinatus tendons will exhibit structural changes compared with macroscopically normal tendons that are progressive with increasing tear size, and that SCI-treatment and SAD surgery influence the structural characteristics of partially-torn human tendons early after treatment.
Materials and Methods
Sample collection
Informed consent and institutional ethical approvals for the use of all samples used in this study were obtained prior to the study. Tendon biopsies from the lateral torn edge of 33 rotator cuff tendons containing full-thickness tears were collected during surgical repair as part of a randomised trial in which patients with full thickness rotator cuff tears were randomly allocated to arthroscopic or open surgical repair groups. Gender differences were not measured. Patients with rotator cuff tears were identified pre-operatively using ultrasound. Intra-operatively, the size of the rotator cuff tear was measured as the anteroposterior dimension of the tear and classified as small (< 1 cm, n = 9), medium (1cm to 3 cm, n = 7), large (3 cm to 5 cm, n = 6) or massive (> 5cm, n = 11). Control biopsies (n = 5) were obtained from the subscapularis tendon of patients undergoing hemiarthroplasty of the shoulder when the tendons appeared macroscopically normal. The inclusion and exclusion criteria for this study are detailed inTable I.
Table I
Inclusion and exclusion criteria for patients recruited to surgical repair cohort
| Inclusion criteria: all of the following must apply |
|---|
| Male or female |
| Over 50 years old |
| Degenerative rotator cuff tear |
| Full thickness rotator cuff tear |
| Diagnosed using MRI or ultrasound |
| Able to consent |
| Exclusion criteria: none of the following may apply: |
| Previous surgery on affected shoulder |
| Dual shoulder pathology |
| History of rheumatoid arthritis/systemic disease |
| Significant osteoarthritis problems |
| Significant neck problems |
| Cognitive impairment/language issues |
Tendon biopsies were also collected from tendons containing partial-thickness tears before and seven weeks after SCI treatment (n = 11), and before and seven weeks after SAD surgery (n = 14). These samples were collected as part of an observational cohort study of patients undergoing treatment for rotator cuff pathology. The seven-week time point was dictated by clinical follow-up restrictions. At both time points, a 14G BARD Magnum™ core biopsy needle (BARD Biopsy, Tempe, Arizona) under ultrasound guidance was used to collect biopsies from the supraspinatus tendon 5 mm posterior to the rotator interval, parallel with the footprint of the tendon as close to the enthesis, with the post-treatment biopsy collected within close proximity of the pre-treatment biopsy. Control biopsies (n = 16) were obtained from the supraspinatus tendon of patients without a history of rotator cuff problems or SCIs, during anterior stabilisation of the shoulder where the tendons appeared macroscopically normal. The inclusion and exclusion criteria for this study are detailed in Table II and Table III summarises the clinical data for all of the samples used in the present study.
Table II
Inclusion and exclusion criteria for patients recruited to serial biopsy study
| Inclusion Criteria: all of the following must apply |
|---|
| Male or female |
| Between 35 and 65 years old |
| Diagnosed with subacromial impingement OR partial thickness rotator cuff tear |
| Referred to secondary care for management of rotator cuff pathology |
| Symptom duration > three months |
| Planning to have glucocorticoid injection or subacromial decompression surgery as a treatment intervention |
| Able to consent |
| Exclusion Criteria: none of the following may apply: |
| More than three previous glucocorticoid injections to the affected shoulder |
| Glucocorticoid injection to the affected shoulder within six weeks prior to intervention |
| History of significant trauma, surgery, osteoarthritis or other pathology of the affected shoulder unrelated to the rotator cuff |
| Allergy/hypersensitivity to lidocaine local anaesthetic |
| Meet the exclusion criteria for administration of SonoVue™ contrast agent (Bracco Imaging, Monroe Township, New Jersey) |
| Any other factor that could jeopardise the safe and ethical conduct of participant care, study operations or other research projects |
Table III
Clinical data for samples characterised in the current study
| Cohort | Number of patients | Mean age (range) | Number of patients having had one or more previous steroid injections (%) | Gender (M:F) | Collection method | ||
|---|---|---|---|---|---|---|---|
| Control (supraspinatus) | 5 | 74.6 (64 to 83) | Unknown | 2:3 | Intra-operative (hemiarthroplasty) | ||
| Control (subscapularis) | 16 | 23.3 (17 to 29) | 0 | 14:2 | Intra-operative (anterior stabilisation) | ||
| Partial tear (subacromial corticosteroid injections) | 11 | 51.5 (35 to 64) | 6 (55) | 4:7 | Ultrasound-guided biopsy | ||
| Partial tear (subacromial decompression surgery) | 14 | 49.1 (36 to 61) | 9 (64) | 10:4 | Ultrasound-guided biopsy | ||
| Small tear | 9* | 66.1 (58 to 78) | 4, 1 unknown (≥ 44) | 6:3 | Intra-operative | ||
| Medium tear | 7 | 57.4 (51 to 67) | 5, 1 unknown (≥ 71) | 3:4 | Intra-operative | ||
| Large tear | 6* | 63.7 (60 to 73) | 3, 2 unknown (≥ 50) | 4:2 | Intra-operative | ||
| Massive tear | 11* | 69.0 (61 to 80) | 5, 2 unknown (≥ 45) | 10 male 1 unknown | Intra-operative | ||
-
* Not significantly different to subscapularis control
Sample preparation
After collection, all samples were fixed in 10% formalin, dehydrated through graded industrial methylated spirit (IMS) (70%, 90%, 95%, 100%), immersed in xylene, and perfused and embedded in Formula R paraffin wax (Surgipath Europe Ltd, Peterborough, UK). Sections of 10 μm and 3 μm were cut from each embedded sample and mounted on Xtra glass slides (Surgipath Europe Ltd). Slides were baked at 60°C for 24 hours prior to storage.
Ultra-structural analysis
Prior to AFM imaging, one 10 μm section per sample was dewaxed in xylene for up to two hours and allowed to dry. Sections were then imaged using an AutoProbe AFM (Park Systems, Suwon, Korea) in non-contact mode using a scan rate of 1 Hz and cantilever probes with a tip radius of curvature of approximately 10 nm, force constant between 4.5 Nm-1 and 14.0 Nm-1 (μmasch, Tallinn, Estonia). A total of six 3 µm x 3 µm images from different locations were obtained from each sample and analysed to measure the fibril diameter of, and mean angle between, 5 and 10 fibrils within each image (Fig. 1). A total of six 3 µm x 3 µm images from different locations were obtained from each sample and analysed to measure the fibril diameter of, and mean angle between, 5 and 10 fibrils within each image (Fig. 1) using Gwyddion v2.23 SPM Data Visualisation and Analysis software (open-source software for SPM data analysis, available at http://gwyddion.net/). Imaging and analysis was performed blind.
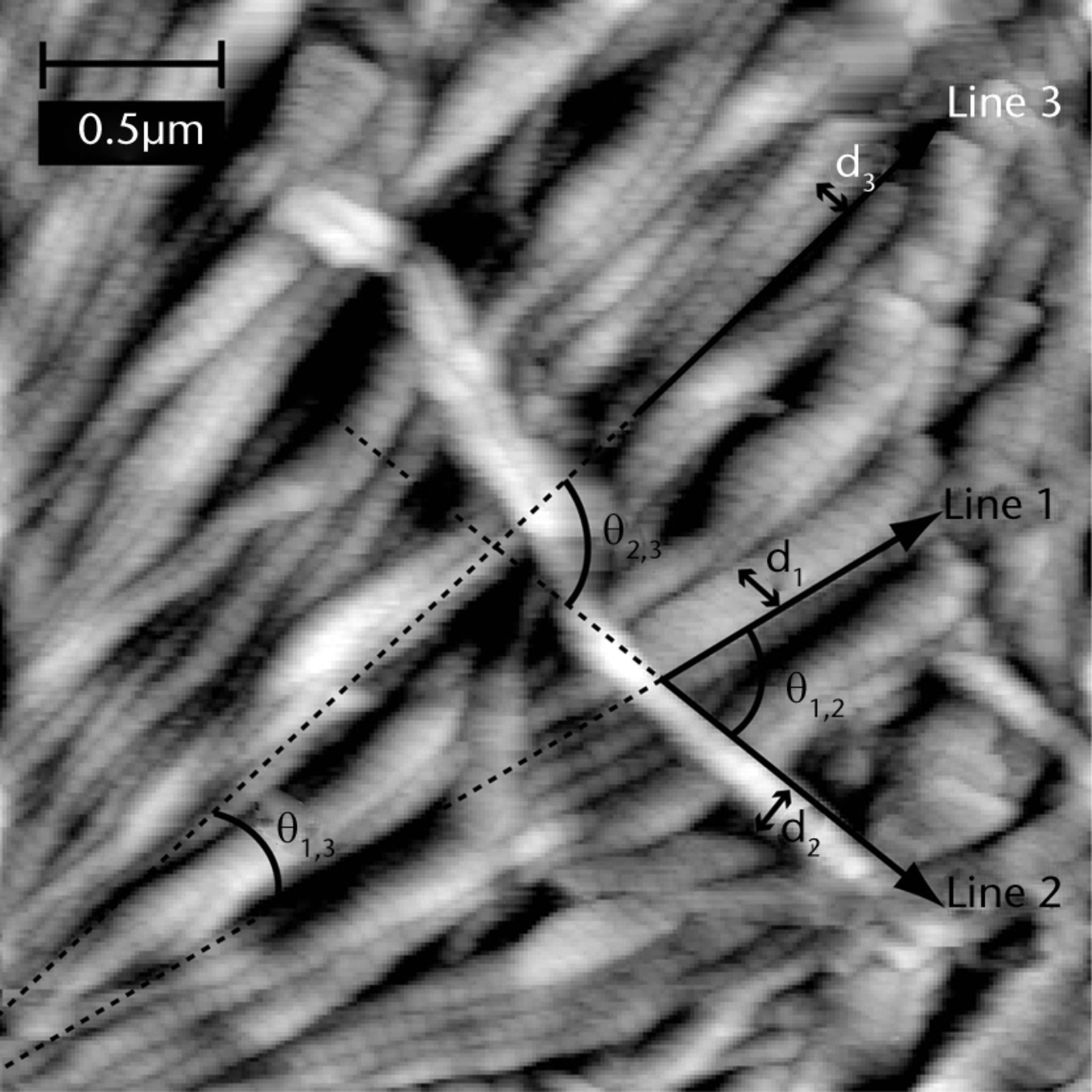
Fig. 1
Representative AFM image of supraspinatus control tendon annotated to illustrate measurement of the diameters of (d1, d2 and d3) and the angles between (θ1,2, θ2,3 and θ1,3) three fibrils. Similar measurements were performed for 10 fibrils in each image.
Micro-structural analysis
Prior to polarised light microscopy imaging, one 3 μm section from each sample was dewaxed in xylene, rehydrated through graded IMS and distilled water and immersed in picrosirius red solution (0.5 g Sirius red F3B in 500 ml saturated aqueous picric acid) (Sigma Aldrich, Dorset, UK) for one hour, rinsed in 0.5% acetic acid, dehydrated through graded IMS, cleared in xylene and mounted in DPX mounting media. Stained samples were imaged in three locations with polarised light microscopy in transmission mode using a Polyvar Met microscope (Reichert-Jung, Depew, New York) fitted with a DFC 420 digital camera (Leica Camera AG, Solms, Germany). The contrast mechanism by which picrosirius red staining of collagen produces this range of colours is not fully understood, however fibres which appear red can generally be considered to be thicker in diameter than those which appear orange.43 The ratio of thick (red) to thin (orange) fibres in each image (Fig. 2) to thin (orange) fibres in each image (Fig. 2) fibres in each image (Fig. 2) was analysed by the use of a threshold colour plug-in for ImageJ (US National Institutes of Health, Bethesda, Maryland) to extract the percentage area of each image that contained different hues. The corresponding histograms were then analysed using OriginPro data analysis software (OriginLab, Northampton, USA) to calculate the ratios of the red and orange peak integrals in each histogram. ImageJ was also used to measure the average crimp length within each picrosirius red-stained sample, based on at least 25 measurements per image.
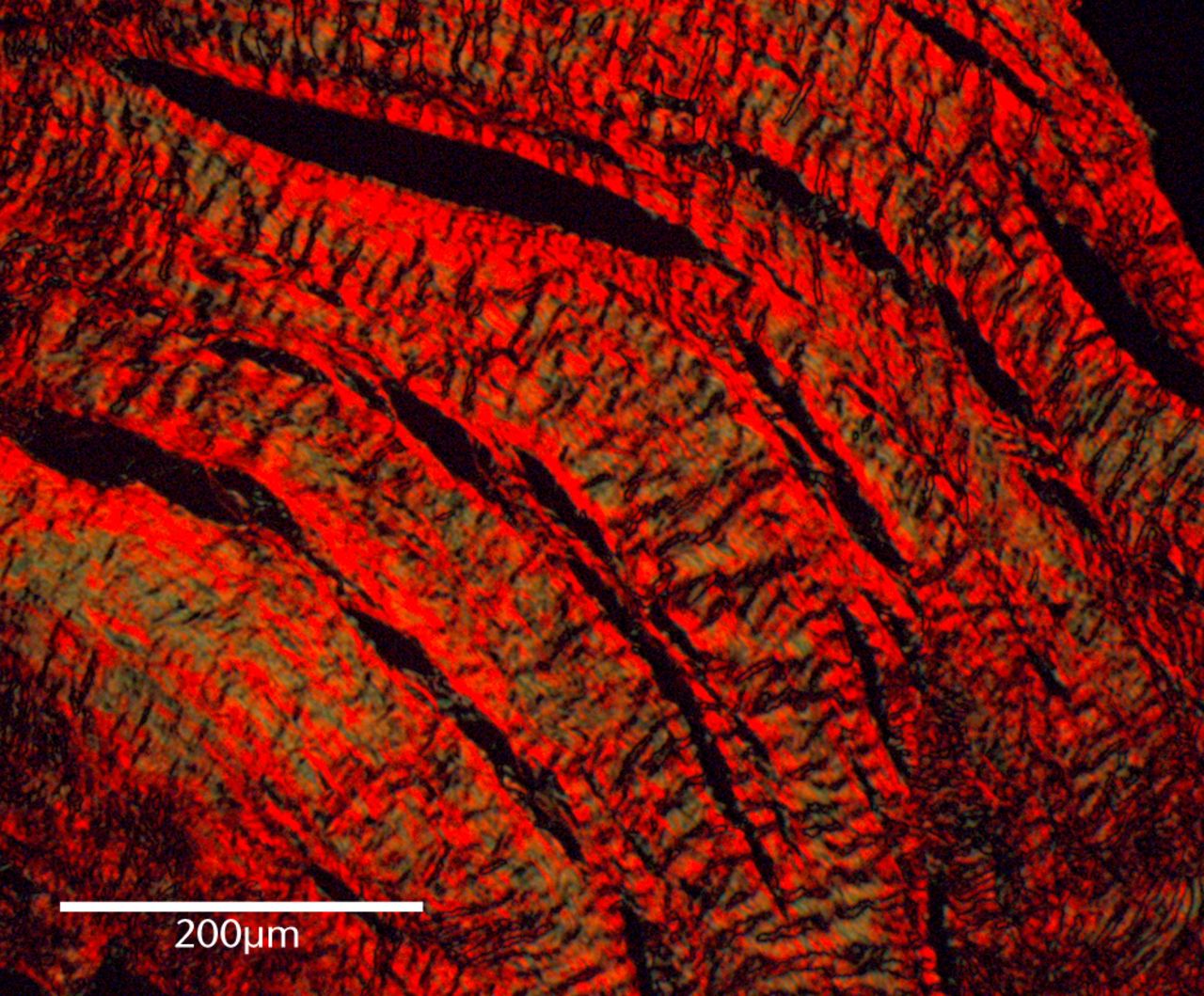
Fig. 2
Representative polarised light microscopy image of a picrosirius-stained supraspinatus control tendon.
Statistical analysis
Power analysis, assessed using ‘R’ Biostatistical analysis freeware (R Development Core Team, www.r-project.org) and based on preliminary experiments, revealed that a minimum of five samples was needed in order to distinguish differences of 1 standard deviation in fibril diameter at p < 0.05 statistical significance and 80% confidence level. Data is presented as box and whisker plots in which the end of the box represents the 25th and 75th percentiles (inter-quartile range), the end of the whisker represents the 5th and 95th percentiles respectively, and mean and median are indicated. Since the data set in the current study was non-orthogonal, it was not possible to account for patient age in two-way ANOVA statistical tests (such tests are only valid for balanced, or near-proportional experimental setups). Statistical significance compared with controls was therefore evaluated using one-way analysis of variance (ANOVA) and Tukey’s multiple comparison test performed using OriginPro data analysis software (OriginLab, Northampton, Massachusetts). Patient age was included as a confounding factor in multivariate linear regression analysis performed using ‘R’ Biostatistical analysis freeware (R Foundation for Statistical Computing, Vienna, Austria). A significance level of p < 0.05 was considered statistically significant.
Results
Structural characteristics across the disease spectrum
Torn tendons were structurally different to the supraspinatus (young) control group but only with a larger mean angle between fibrils in the medium and massive full thickness tear groups (Fig. 3) control group but only with a larger mean angle between fibrils in the medium and massive full thickness tear groups (Fig. 3), and a shorter crimp length in the small full thickness tear group.
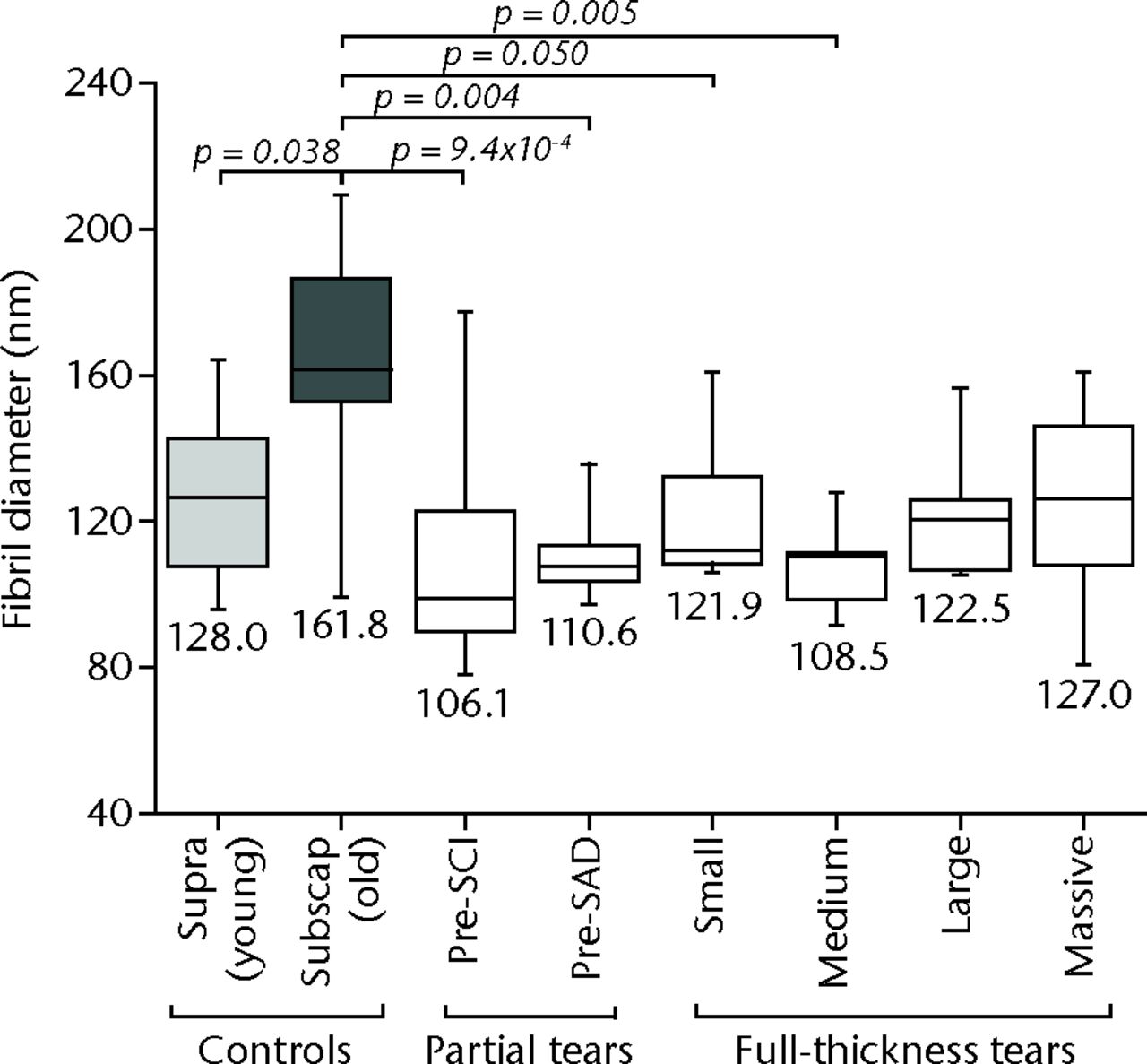
Fig. 3
Graph showing the mean angle between fibrils measurements for different tear-size groups compared with supra(spinatus) (young) and subscap(ularis) (old) control groups. Significant differences exist between medium (p = 0.017) and massive (p = 0.010) tear groups compared with the subscapularis control group.
Greater differences were found between the torn groups and the subscapularis (old) control groups, with torn tendons exhibiting significantly thinner fibrils (Fig. 4) control groups, with torn tendons exhibiting significantly thinner fibrils (Fig. 4), lower ratios of thick-to-thin fibres (Fig. 5), and shorter crimp lengths (Fig. 6) compared with the subscapularis (old) controls. These differences were first evident in partial tear groups for fibril-diameter data (Fig. 4) controls. These differences were first evident in partial tear groups for fibril-diameter data (Fig. 4), and in the small full thickness tear group for ratio of thick-to-thin fibres and crimp-length data (Figs 5 and 6).
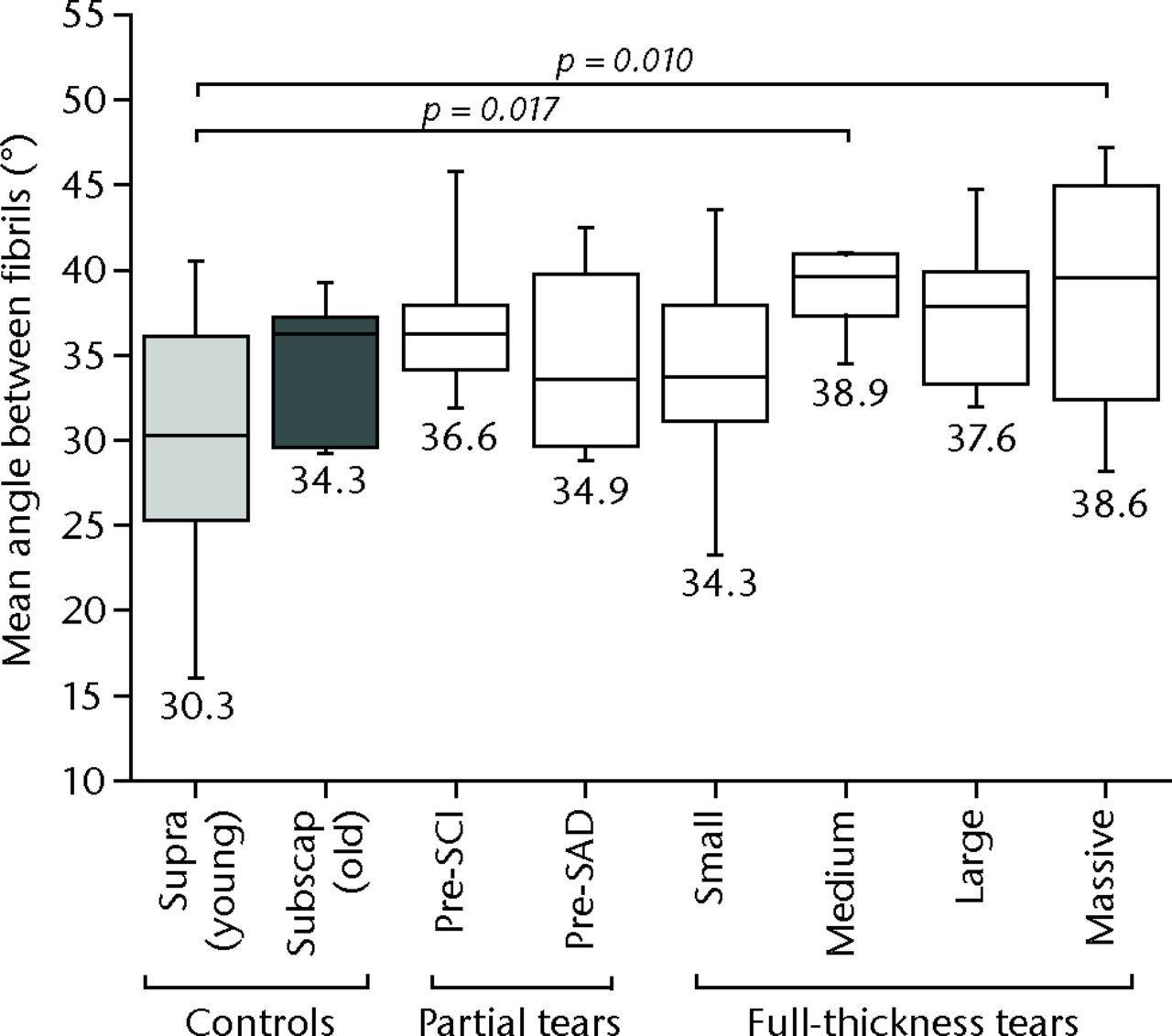
Fig. 4
Fibril diameter measurements for different tear size groups compared with supras(pinatus) (young) and subscap(ularis) (old) control groups. Significant differences exist between tear groups and the control groups, although there are more differences compared with the subscapularis control group than the supraspinatus controls.
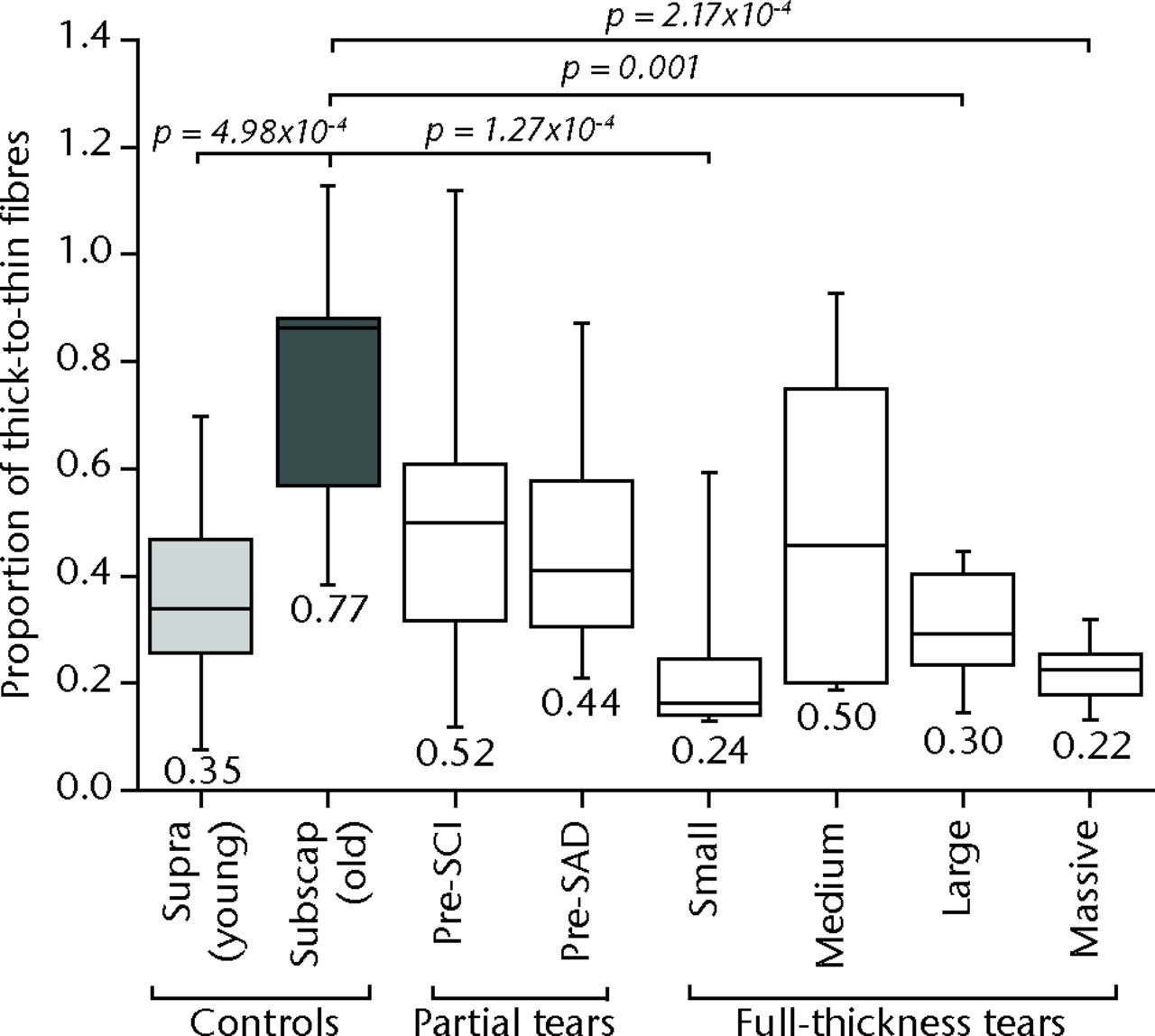
Fig. 5
Ratio of thick-to-thin fibres for different tear size groups compared with supra(spinatus) (young) and subscap(ularis) (old) control groups. Significant differences exist between the two control groups, and between small, large and massive tear groups compared with the supraspinatus control group.
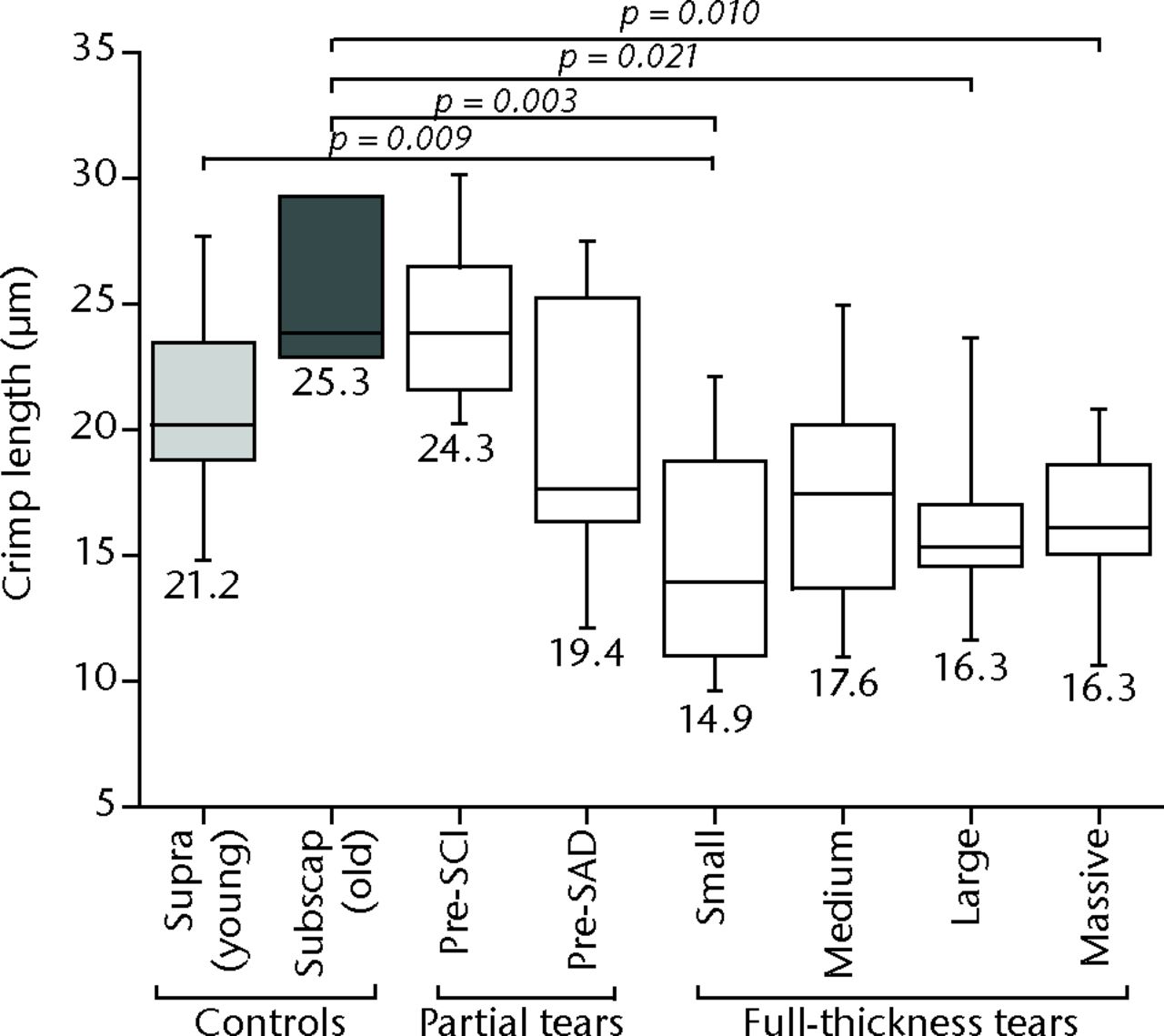
Fig. 6
Crimp length measurements for different tear size groups compared with supra(spinatus) (young) and subscap(ularis) (old) control groups. Significant differences exist between the two control groups, and between small, large and massive tear groups compared with the supraspinatus control group.
Significant structural differences were also found between the two control groups; the supraspinatus (young) control group exhibited significantly thinner fibrils (p = 0.038) (Fig. 4) control group exhibited significantly thinner fibrils (p = 0.038) (Fig. 4) (Fig. 4) and a significantly lower ratio of thick-to-thin fibres (p = 4.98x10-4) (Fig. 5) (Fig. 5) than the subscapularis (old) control group. The supraspinatus (young) control group also exhibited a smaller mean angle between fibrils (Fig. 3) control group. The supraspinatus (young) control group also exhibited a smaller mean angle between fibrils (Fig. 3) control group also exhibited a smaller mean angle between fibrils (Fig. 3) and shorter crimp lengths (Fig. 6) compared with the subscapularis (old) control group, although these differences were not significant (p > 0.05).
Relationship with increasing tear size
Significant linear regression models were found for decreasing crimp length with increasing tear size using the supraspinatus (young) control group, and for decreasing fibril diameter, decreasing ratio of thick-to-thin fibres and decreasing crimp length using the subscapularis (old) control group (Table IV), although the correlations were weak (R2 < 0.5). Regardless of the control group used in the analysis, patient age was not a significant explanatory variable in the models, with the exception of fibril diameter using the subscapularis (old) control group.
Table IV
Descriptive statistics for multivariate linear regression models describing changes in structural characteristics with increasing tear size using different control groups
| Intercept | Slope, β | Probability, p | R2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| β tear size | β age | p tear size | p age | p overall | |||||||
| Fibril diameter | |||||||||||
| Supraspinatus control | 116.2 | 0.638 | -0.003 | 0.798 | 0.991 | 0.899 | 0.003 | ||||
| Subscapularis control | 70.0 | -3.328 | 1.082 | 0.059 | 5.90x10-5 | 2.873 x10-4 | 0.257 | ||||
| Mean angle between fibrils | |||||||||||
| Supraspinatus control | 34.3 | 1.250 | -0.062 | 0.067 | 0.504 | 0.120 | 0.081 | ||||
| Subscapularis control | 32.6 | 0.749 | 0.009 | 0.092 | 0.889 | 0.162 | 0.064 | ||||
| Ratio of thick-to-thin fibres | |||||||||||
| Supraspinatus control | 0.41 | -0.054 | 0.004 | 0.086 | 0.317 | 0.062 | 0.154 | ||||
| Subscapularis control | 0.64 | -0.076 | 0.002 | 0.001 | 0.574 | 0.002 | 0.213 | ||||
| Crimp length | |||||||||||
| Supraspinatus control | 24.3 | -0.730 | -0.052 | 0.138 | 0.369 | 3.69 x 10-4 | 0.222 | ||||
| Subscapularis control | 26.0 | -1.329 | -0.028 | 0.001 | 0.605 | 3.38 x 10-4 | 0.260 | ||||
Early influence of tendinopathy treatments
With the exception of a significantly smaller mean angle between fibrils in samples post-SAD surgery compared with samples pre-SAD surgery (p = 0.005), there were no significant differences between the structural characteristics of the tendons before, compared with that following, intervention (p > 0.05) (Figs. 7 to 10).
Discussion
The aetiology and pathology of rotator cuff tendinopathy is unclear. However, various studies have suggested that this disease is associated with tissue degeneration, which may be progressive with increasing tear size.12,13,44 The structural changes of torn human rotator cuff tendons have not previously been characterised across the full disease spectrum because previous sampling limitations have restricted the collection of samples in human cuff tendons containing partial thickness tears. Similarly, the effects of common cuff tendinopathy treatments, such as SCI and SAD surgery, on the structural properties of partially torn human rotator cuff tendons in vivo have not been definitively investigated. The present study has used a minimally invasive biopsy technique to quantitatively evaluate the structural characteristics of human rotator cuff tendons across the full spectrum of disease for the first time. Using this technique, we have gained novel insight into the strong correlation between increasing tear size and degenerative changes within the tissue, as well as the efficiency of common tendinopathy treatments for arresting and reversing degenerative structural changes in the initial stages of disease.
In agreement with previous studies,45-47 our study demonstrates that torn supraspinatus tendons exhibit significantly thinner fibrils (Fig. 4), higher proportions of thinner fibres (indicated by lower ratios of thick-to-thin fibres) (Fig. 5) (Fig. 5), and shorter crimp lengths (Fig. 6) compared with control samples. Importantly, the inclusion of partially torn tendons in the present study provides a more complete view of disease progression across the entire disease spectrum than has previously been available.48,49 This has enabled us to demonstrate the existence of structural changes much earlier in the progression of disease than has previously been possible (i.e. in tendons containing partial thickness and small full thicknesses tears), and to provide further evidence of a progressive relationship between increasing tear size and degenerative changes in torn cuff tendons. The existence of structural differences early in the disease spectrum that appear to increase as tear size increases, have important implications for the timing of clinical intervention strategies. Specifically, these results suggest that any intervention strategy should be performed as early as possible in the progression if it is to arrest, or even reverse, the degenerative changes associated with increasing tear size.13,50
To date, the ability of common clinical intervention strategies to arrest, or reverse, the degenerative changes exhibited by torn tissue have not been fully investigated owing to a lack of methodologies capable of collecting tissue samples before and after intervention. In this study we have used a novel methodology for serial collection of tissue samples before and after intervention in order to assess, for the first time, the efficiency of two current clinical intervention strategies for rotator cuff tendinopathy, SCI treatment and SAD surgery.23
The influence of SCIs and SAD on the structural properties of partially torn tendon tissue is largely unknown. While neither of these strategies aims to alter the structure of the cuff tendon directly, previous studies suggest that the structural properties of partially torn supraspinatus tendons may be altered by both interventions. SCI treatment has been shown to cause necrosis, tissue degeneration and reduced mechanical properties – characteristics commonly associated with structural alterations – in healthy and released animal models within two weeks of treatment.25,51 Conversely, randomised placebo controlled trials have demonstrated functional improvement within four weeks of treatment, possibly indicating increased tissue integrity (and altered structural properties).23 Similarly, patients who have undergone SAD surgery have been shown to exhibit significant functional improvements three weeks post-intervention.26,52 Our findings, however, provide no evidence to suggest that either SCI or SAD-treated partially torn supraspinatus tendons exhibited any significant structural changes seven weeks after treatment, with the exception of a decrease in mean angle between fibrils post-SAD (Figs 7 to 10). While this finding is unsurprising given the relatively slow collagen remodelling process within tendon,53 it indicates that functional recovery does not necessarily equate to recovery of tissue properties.
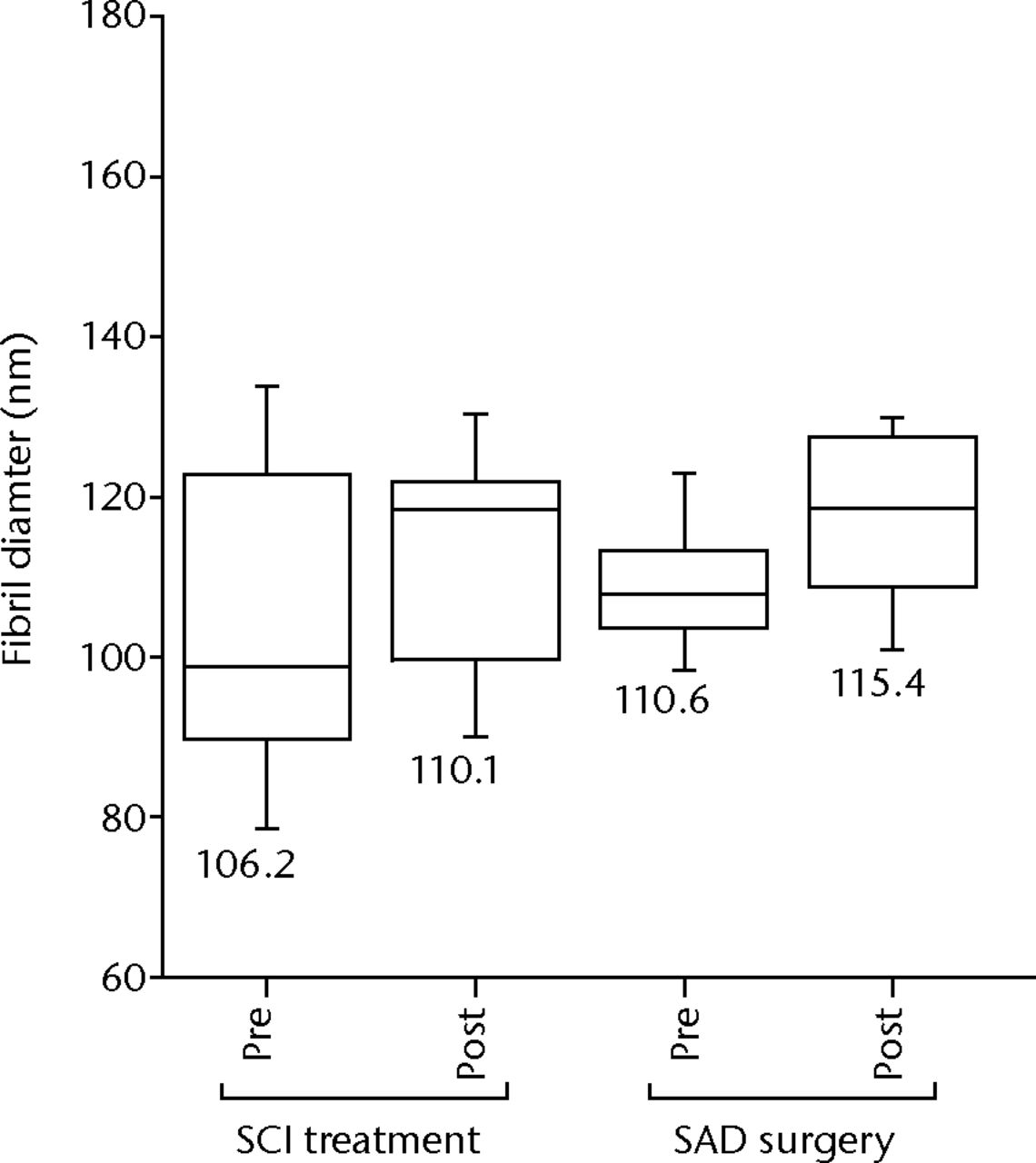
Fig. 7
Fibril diameter measurements for partial tear groups before and after subachromial corticosteroid injections (SCI) and subacromial decompression (SAD) treatments. There are no significant changes in fibril diameter post-SCI treatment or post-SAD surgery compared with the pre-treatment measurements (p > 0.05).
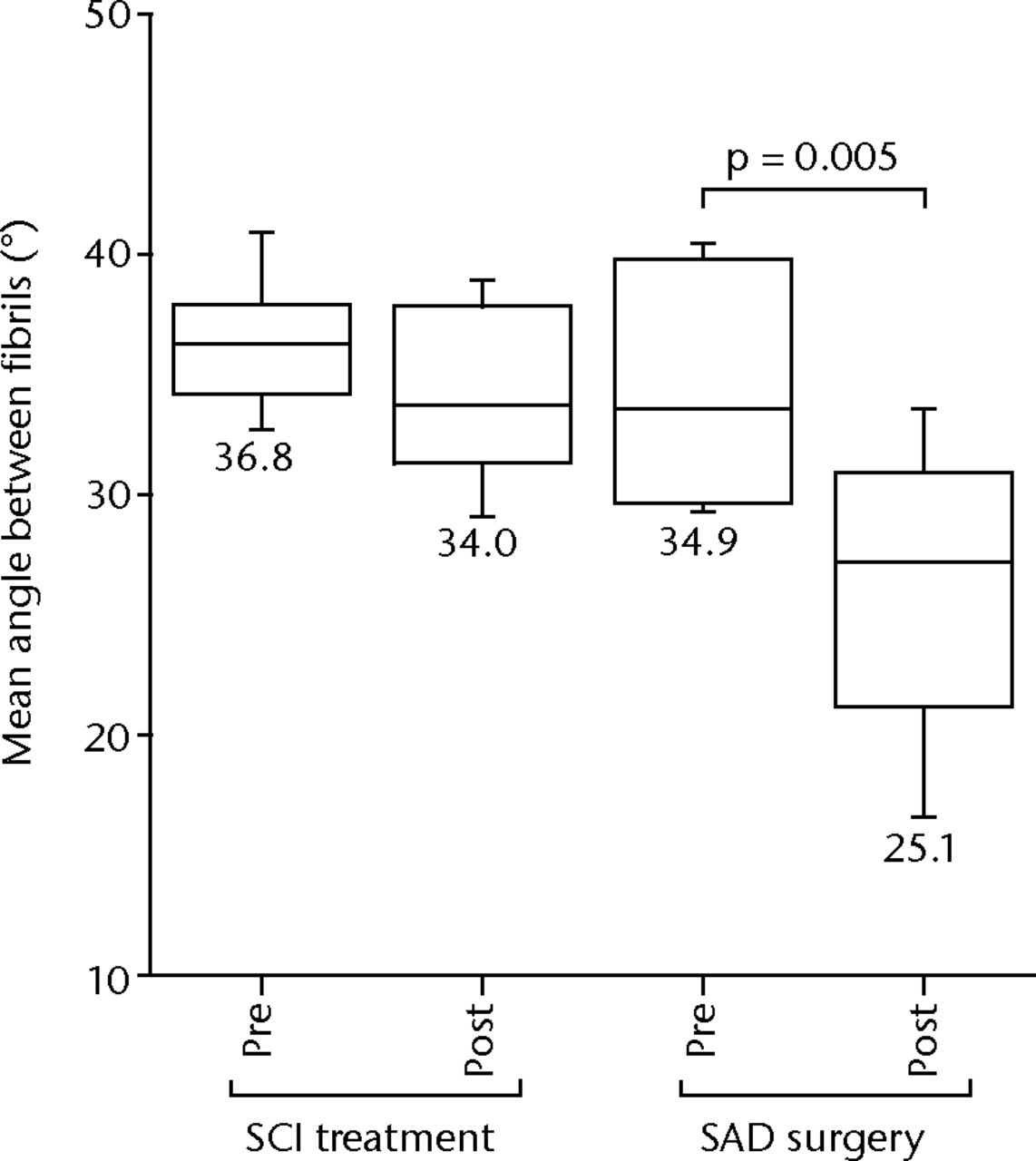
Fig. 8
Mean angle between fibril measurements for partial tear groups before and after subachromial corticosteroid injections (SCI) and subacromial decompression (SAD) treatments. There are no significant changes in mean angle post- SCI treatment. There is a significant decrease in mean angle post-SAD surgery compared with the pre-SAD-surgery measurements (p = 0.005).
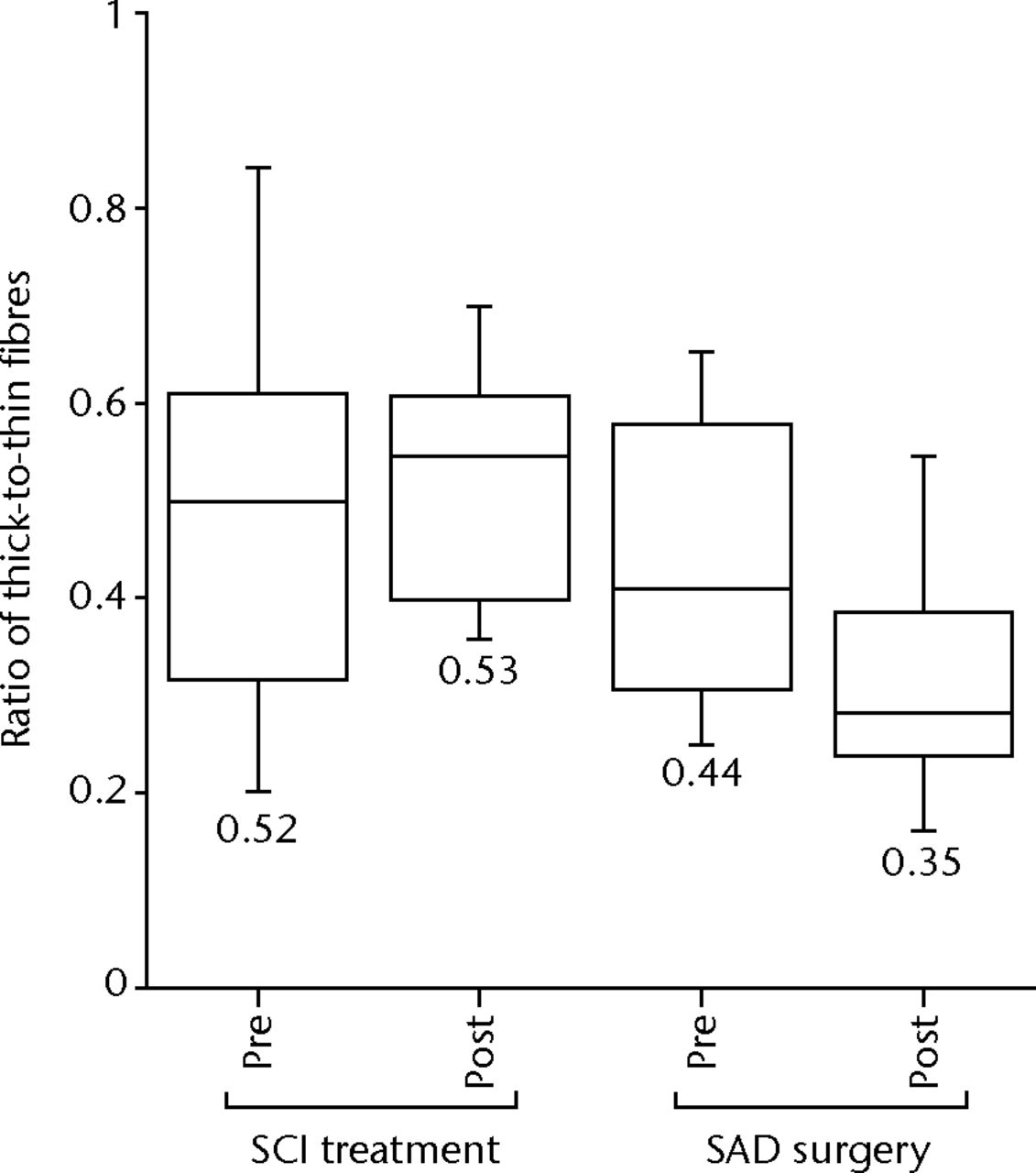
Fig. 9
Ratio of thick-to-thin fibres measurements for partial tear groups before and after subachromial corticosteroid injections (SCI) and subacromial decompression (SAD) surgery. There are no significant changes in the ratio of thick-to-thin fibres after SCI-treatment or after SAD surgery compared with the pre-treatment measurements (p > 0.05).
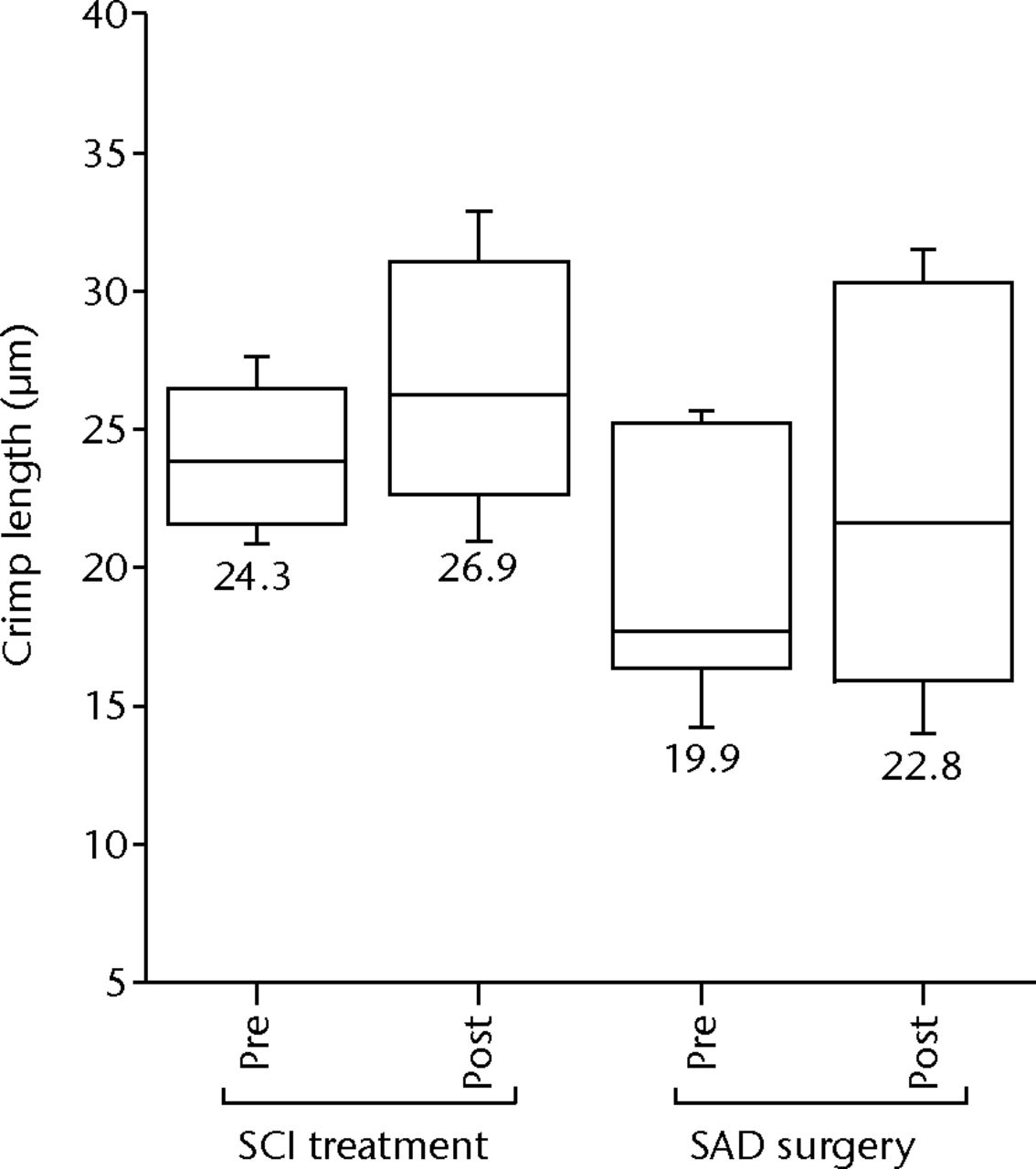
Fig. 10
Crimp length measurements for partial tear groups before and after subachromial corticosteroid injections (SCI) and subacromial decompression (SAD) surgery. There are no significant changes in crimp length after SCI treatment or after SAD surgery compared with the pre-treatment measurements (p > 0.05).
In addition to revealing important information regarding the structural properties of torn rotator cuff tendons, our results emphasise the importance of the correct choice of control tissue. The weight of evidence to support our conclusions is much greater when the structural characteristics of the torn groups are compared with the old subscapularis tendon control group than with the young supraspinatus tendon control group, and significant structural differences were found between the two control groups (Figs 3 to 6). These differences are likely associated with differences in 1) tissue source (subscapularis versus supraspinatus tendon) and 2) patient age between the two groups, both of which influence the structural properties of tendons.5,54,55 Both characteristics should therefore be considered when selecting a control group. However, as it is rarely possible to match both age and tissue in control tissue, compromises are often made.
In rotator cuff studies, the strong correlation between the incidence of rotator cuff tears and the age of the patient5 has resulted in a pronounced lack of age-matched, macroscopically normal supraspinatus tendons available for use as control tissue. Consequently, many studies have relied on an age-matched subscapularis tendon or an older cadaveric supraspinatus tendon as control material instead.13,56,57 Given the significant differences between the structural properties of young supraspinatus tendon and old subscapularis tendon found in the current study (Figs 3 to 6), such tissue may not best represent the properties of healthy supraspinatus tendon tissue. While this may have some implications for the interpretation of their results, however, it is unlikely to invalidate the findings of the present study as significant differences were detected in the torn group regardless of the control group used (Figs 3 to 6).
There are two limitations of this study which should be acknowledged. Firstly, the samples obtained as part of the surgical study were collected from the lateral torn edge of the supraspinatus tendon, whereas the samples obtained as part of the serial biopsy study were collected from tendons that remained in continuity with the bone. Given the importance of topology indicated by cadaveric and biopsy studies performed by our research group (unpublished), this is could give rise to some variability within the data, although this is not expected to be significant. Secondly, while this pilot study has not demonstrated any structural changes in tendons containing partial thickness tears seven weeks after SCI or SAD surgery, this time scale may not be a sufficient for structural adaptations. However, having demonstrated the power of this minimally invasive biopsy technique for collecting serial pre- and post-intervention samples, it is hoped that future studies will build upon these results, with clinical follow-up over longer timescales and investigations into the efficiency of additional interventions.
In conclusion, this study has used a novel, minimally invasive biopsy technique in order to evaluate the structural characteristics of torn human supraspinatus tendons across the full disease spectrum, and the short-term effects of SCIs and SAD surgery on these structural characteristics. Our findings provide evidence that torn rotator cuff tendons exhibit structural changes compared with macroscopically normal tendons that occur early in the disease spectrum and are progressive with increasing tear size. Neither SCIs nor SAD surgery alter these structural changes in partially-torn rotator cuff tendons, with the exception of a decrease in the mean angle between fibrils post- compared with pre-SAD surgery.
These findings are of great clinical relevance, particularly with respect to 1) the timing of clinical interventions, with our findings suggesting that the timing of clinical intervention may be key for preventing further degeneration of the tissue, 2) the nature of the intervention, with the findings suggesting that neither SCI nor SAD surgery are capable of reversing the degenerative changes exhibited by torn cuff tendons in the short term and 3) the demonstration of a powerful methodology that opens the way for assessing the effect of different intervention strategies on tissue characteristics. Future work should now use the minimally invasive sampling technique to focus on the development and evaluation of strategies for detecting and reversing these pathological adaptations early in the progression of disease, in order to prevent further tissue degeneration associated with increasing tear size.
Acknowledgements: The authors would like to acknowledge Oxford Musculoskeletal Biobank for assistance with sample acquisition and Prof. C. Governor for provision of laboratory space.
1 Bureau of Labor Statistics. Nonfatal Occupational Injuries and Illnesses Requiring Days Away from Work, 2007 https:// http://www.bls.gov/ (date last accessed 09 June 2014). Google Scholar
2 Jacobsson L , LindgärdeF, ManthorpeR. The commonest rheumatic complaints of over six weeks' duration in a twelve-month period in a defined Swedish population. Prevalences and relationships. Scand J Rheumatol1989;18:353–360.CrossrefPubMed Google Scholar
3 Ostör AJ , RichardsCA, PrevostAT, SpeedCA, HazlemanBL. Diagnosis and relation to general health of shoulder disorders presenting to primary care. Rheumatology (Oxford)2005;44:800–805.CrossrefPubMed Google Scholar
4 Allander E . Prevalence, incidence, and remission rates of some common rheumatic diseases or syndromes. Scand J Rheumatol1974;3:145–153. Google Scholar
5 Brewer BJ . Aging of the rotator cuff. Am J Sports Med1979;7:102–110.CrossrefPubMed Google Scholar
6 Bloom DE, Canning D. Global Demographic Change: Dimensions and Economic Significance: National Bureau of Economic Research Working Paper Series 2004 No. 10817. http://www.nber.org/ (date last accessed 09 June 2014). Google Scholar
7 Fehringer EV , SunJ, VanOeverenLS, KellerBK, MatsenFA 3rd. Full-thickness rotator cuff tear prevalence and correlation with function and co-morbidities in patients sixty-five years and older. J Shoulder Elbow Surg2008;17:881–885.CrossrefPubMed Google Scholar
8 Järvinen M , JózsaL, KannusP, et al.Histopathological findings in chronic tendon disorders. Scand J Med Sci Sports1997;7:86–95.CrossrefPubMed Google Scholar
9 Yuan J , MurrellG, WeiA, WangM. Apoptosis in Rotator Cuff Tendonopathy. J Orthop Res2002;20:1372–1379.CrossrefPubMed Google Scholar
10 Hashimoto T , NobuharaK, HamadaT. Pathologic evidence of degeneration as a primary cause of rotator cuff tear. Clin Orthop Relat Res2003;415:111–120.CrossrefPubMed Google Scholar
11 Benson RT , McDonnellSM, KnowlesHJ, et al.Tendinopathy and tears of the rotator cuff are associated with hypoxia and apoptosis. J Bone Joint Surg [Br]2010;92-B:448–453.CrossrefPubMed Google Scholar
12 Shindle MK , ChenCC, RobertsonC, et al.Full-thickness supraspinatus tears are associated with more synovial inflammation and tissue degeneration than partial-thickness tears. J Shoulder Elbow Surg2011;20:917–927.CrossrefPubMed Google Scholar
13 Matthews TJ , HandGC, ReesJL, AthanasouNA, CarrAJ. Pathology of the torn rotator cuff tendon. Reduction in potential for repair as tear size increases. J Bone Joint Surg [Br]2006;88-B:489–495.CrossrefPubMed Google Scholar
14 Williams LN , ElderSH, HorstemeyerMF, HarbargerD. Variation of diameter distribution, number density, and area fraction of fibrils within five areas of the rabbit patellar tendon. Ann Anat2008;190:442–451.CrossrefPubMed Google Scholar
15 Wilson C , DuffG. Pathological study of degeneration and rupture of the supraspinatus tendon. Arch Surg 1943;47:121–135. Google Scholar
16 Attia M , ScottA, DuchesnayA, et al.Alterations of overused supraspinatus tendon: a possible role of glycosaminoglycans and HARP/pleiotrophin in early tendon pathology. J Orthop Res2012;30:61–71.CrossrefPubMed Google Scholar
17 Longo UG , FranceschiF, RuzziniL, et al.Light microscopic histology of supraspinatus tendon ruptures. Knee Surg Sports Traumatol Arthrosc2007;15:1390–1394.CrossrefPubMed Google Scholar
18 Chaudhury S , HollandC, VollrathF, CarrAJ. Comparing normal and torn rotator cuff tendons using dynamic shear analysis. J Bone Joint Surg [Br]2011;93-B:942–948.CrossrefPubMed Google Scholar
19 Tillander B , FranzénL, NorlinR. Fibronectin, MMP-1 and histologic changes in rotator cuff disease. J Orthop Res2002;20:1358–1364.CrossrefPubMed Google Scholar
20 Sano H , IshiiH, TrudelG, UhthoffHK. Histologic evidence of degeneration at the insertion of 3 rotator cuff tendons: a comparative study with human cadaveric shoulders. J Shoulder Elbow Surg1999;8:574–579.CrossrefPubMed Google Scholar
21 Chaudhury S , GwilymSE, MoserJ, CarrAJ. Surgical options for patients with shoulder pain. Nat Rev Rheumatol2010;6:217–226.CrossrefPubMed Google Scholar
22 Murphy RJ, Carr AJ. Shoulder pain. Clin Evid (Online) 2010;pii:1107. Google Scholar
23 Green S, Buchbinder R, Glazier R, Forbes A. Interventions for shoulder pain. Cochrane Database Syst Rev 2000;2:CD001156. Google Scholar
24 Björkenheim JM , PaavolainenP, AhovuoJ, SlätisP. Surgical repair of the rotator cuff and surrounding tissues. Factors influencing the results. Clin Orthop Relat Res1988;236:148–153.PubMed Google Scholar
25 Mikolyzk DK , WeiAS, ToninoP, et al.Effect of corticosteroids on the biomechanical strength of rat rotator cuff tendon. J Bone Joint Surg [Am]2009;91-A:1172–1180.CrossrefPubMed Google Scholar
26 Dodenhoff R , McLellandD. Rate of Recovery after Arthroscopic Subacromial Decompression for Shoulder Impingement Syndrome. J Bone Joint Surg [Br]2002; 84-B(SII):194–194. Google Scholar
27 Longo UG , OlivaF, DenaroV, MaffulliN. Oxygen species and overuse tendinopathy in athletes. Disabil Rehabil2008;30:1563–1571.CrossrefPubMed Google Scholar
28 Parry DA , CraigAS, BarnesGR. Tendon and ligament from the horse: an ultrastructural study of collagen fibrils and elastic fibres as a function of age. Proc R Soc Lond B Biol Sci1978;203:293–303.CrossrefPubMed Google Scholar
29 Parry DA , CraigAS. Quantitative electron microscope observations of the collagen fibrils in rat-tail tendon. Biopolymers1977;16:1015–1031.CrossrefPubMed Google Scholar
30 Hayat M . Glutaraldehyde: role in electron microscopy. Micron and Microscopica Acta1986;17:115–135. Google Scholar
31 Dawson IM . Fixation: what should the pathologist do?Histochem J1972;4:381–385.CrossrefPubMed Google Scholar
32 Tromans WJ , HorneRW, GreshamGA, BaileyAJ. Electron microscope studies on the structure of collagen fibrils by negative staining. Z Zellforsch Mikrosk Anat1963;58:798–802.CrossrefPubMed Google Scholar
33 Gotoh T , SugiY. Electron-microscopic study of the collagen fibrils of the rat tail tendon as revealed by freeze-fracture and freeze-etching techniques. Cell Tissue Res1985;240:529–534.CrossrefPubMed Google Scholar
34 Eyden B , TzaphlidouM. Structural variations of collagen in normal and pathological tissues: role of electron microscopy. Micron2001;32:287–300.CrossrefPubMed Google Scholar
35 Feitosa VL , ReisFP, EsquisattoMA, et al.Comparative ultrastructural analysis of different regions of two digital flexor tendons of pigs. Micron2006;37:518–525.CrossrefPubMed Google Scholar
36 Kongsgaard M , QvortrupK, LarsenJ, et al.Fibril morphology and tendon mechanical properties in patellar tendinopathy: effects of heavy slow resistance training. Am J Sports Med2010;38:749–756.CrossrefPubMed Google Scholar
37 Raspanti M , AlessandriniA, OttaniV, RuggeriA. Direct visualization of collagen-bound proteoglycans by tapping-mode atomic force microscopy. J Struct Biol1997;119:118–122.CrossrefPubMed Google Scholar
38 Paige MF , GohMC. Ultrastructure and assembly of segmental long spacing collagen studied by atomic force microscopy. Micron2001;32:355–361.CrossrefPubMed Google Scholar
39 Gutsmann T , FantnerGE, KindtJH, et al.Force spectroscopy of collagen fibers to investigate their mechanical properties and structural organization. Biophys J2004;86:3186–3193.CrossrefPubMed Google Scholar
40 Revenko I , SommerF, MinhDT, GarroneR, FrancJM. Atomic force microscopy study of the collagen fibre structure. Biol Cell1994;80:67–69.CrossrefPubMed Google Scholar
41 Fotiadis D , ScheuringS, MüllerSA, EngelA, MüllerDJ. Imaging and manipulation of biological structures with the AFM. Micron2002;33:385–397.CrossrefPubMed Google Scholar
42 Tilley JM , CarrAJ, CzernuszkaJT. Atomic Force Microscopy of bulk tendon samples: affect of location and fixation on tissue ultrastructure. Micron2011;42:531–535.CrossrefPubMed Google Scholar
43 Rich L , WhittakerP. Collagen and picrosirius red staining: A polarised light assessment of fibrillar hue and spatial distribution. Brazilian Journal of Morphological Sciences2005;22:97–104. Google Scholar
44 Sano H , WakabayashiI, ItoiE. Stress distribution in the supraspinatus tendon with partial-thickness tears: an analysis using two-dimensional finite element model. J Shoulder Elbow Surg2006;15:100–105.CrossrefPubMed Google Scholar
45 Järvinen TA , JärvinenTL, KannusP, JózsaL, JärvinenM. Collagen fibres of the spontaneously ruptured human tendons display decreased thickness and crimp angle. J Orthop Res2004;22:1303–1309.CrossrefPubMed Google Scholar
46 Józsa L , RéffyA, BálintJB. Polarization and electron microscopic studies on the collagen of intact and ruptured human tendons. Acta Histochem1984;74:209–215.CrossrefPubMed Google Scholar
47 Järvinen TA , JärvinenTL, KannusP, JózsaL, JärvinenM. Collagen fibres of the spontaneously ruptured human tendons display decreased thickness and crimp angle. J Orthop Res2004;22:1303–1309.CrossrefPubMed Google Scholar
48 Magnusson SP , QvortrupK, LarsenJO, et al.Collagen fibril size and crimp morphology in ruptured and intact Achilles tendons. Matrix Biol2002;21:369–377.CrossrefPubMed Google Scholar
49 Wang VM , WangFC, McNickleAG, et al.Medial versus lateral supraspinatus tendon properties: implications for double-row rotator cuff repair. Am J Sports Med2010;38:2456–2463.CrossrefPubMed Google Scholar
50 Murphy RJ , KliskeyK, WhewayK, et al.Rotator Cuff Tendinopathy: Immunohistochemical changes across the spectrum of pathology. Br J Sport Med2013;47:2. Google Scholar
51 Akpinar S , HersekliMA, DemirorsH, TandoganRN, KayaselcukF. Effects of methylprednisolone and betamethasone injections on the rotator cuff: an experimental study in rats. Adv Ther2002;19:194–201.CrossrefPubMed Google Scholar
52 Norlin R . Arthroscopic subacromial decompression versus open acromioplasty. Arthroscopy1989;5:321–323.PubMed Google Scholar
53 Kjaer M , LangbergH, HeinemeierK, et al.From mechanical loading to collagen synthesis, structural changes and function in human tendon. Scand J Med Sci Sports2009;19:500–510.CrossrefPubMed Google Scholar
54 Wilmink J , WilsonAM, GoodshipAE. Functional significance of the morphology and micromechanics of collagen fibres in relation to partial rupture of the superficial digital flexor tendon in racehorses. Res Vet Sci1992;53:354–359.CrossrefPubMed Google Scholar
55 Parry DA , BarnesGR, CraigAS. A comparison of the size distribution of collagen fibrils in connective tissues as a function of age and a possible relation between fibril size distribution and mechanical properties. Proc R Soc Lond B Biol Sci1978;203:305–321.CrossrefPubMed Google Scholar
56 Chaudhury S , DickoC, BurgessM, VollrathF, CarrAJ. Fourier transform infrared spectroscopic analysis of normal and torn rotator-cuff tendons. J Bone Joint Surg [Br]2011;93-B:370–377.CrossrefPubMed Google Scholar
57 Riley GP , CurryV, DeGrootJ, et al.Matrix metalloproteinase activities and their relationship with collagen remodelling in tendon pathology. Matrix Biol2002;21:185–195.CrossrefPubMed Google Scholar
Funding statement:
This study was funded by an EPSRC Doctoral Training Studentship and was supported by the National Institute of Health Research Biomedical Research Unit
Author contributions:
J. M. R. Tilley: Sample Preparation, Data collection, Data analysis, Writing the paper, Compiling figures and tables
R. J. Murphy: Performed surgeries
S. Chaudhury: Sample collection
J. T. Czernuszka: Study Overview
A. J. Carr: Performed Surgeries, Study Overview
ICMJE Conflict of Interest:
None declared
©2014 The British Editorial Society of Bone & Joint Surgery. This is an open-access article distributed under the terms of the Creative Commons Attributions licence, which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
